
Back to Annual Meeting Program
CTA-based anatomic evaluation of saphenous vein bypass conduit: utility and correlation with duplex ultrasound.
Dorian J deFreitas1, Timothy P Love1, Karthikeshwar Kasirajan2, Luke P Brewster1, Ravi K Veeraswamy1, Atef Salam2, Joseph J Ricotta, Jr.1, Noel Haskins2, Ron Mixon2, Matthew A Corriere2
1Emory University School of Medicine, Atlanta, GA;2Atlanta VA Medical Center, Atlanta, GA
Background: Lower extremity Computed Tomography Angiography (CTA) is frequently utilized for anatomic assessment of peripheral arterial disease. In patients requiring lower extremity bypass, duplex ultrasound (DUS) is routinely obtained to evaluated great saphenous vein (GSV) for use as conduit. GSV is visible on CTA images but not routinely assessed or included in study interpretation. We hypothesized that CTA images could be used to measure GSV diameters, and that these diameters would correlate with DUS measurements.
Methods- Consecutive patients evaluated preoperatively with both CTA and DUS vein mapping prior to lower extremity bypass were identified at a single hospital. All CTAs were performed using standard protocol without venous phase imaging. Minimum above- and below-knee GSV diameters were independently measured from electronically archived CTA images by two observers. Adequate GSV was defined as minimum DUS diameter ≥3 mm. Reproducibility of CTA-based diameter measurements between observers was evaluated using intraclass correlation coefficients. Correlation between CTA and DUS-based GSV diameters was evaluated with linear regression and Spearman correlation coefficients. Cut-points for identification of adequate GSV bypass conduit using CTA were determined using receiver operating characteristic curves.
Results- Thirty six limbs were evaluated in 27 patients. In the absence of previous surgical removal, GSV was visible on all CTAs reviewed. No instances of GSV thrombosis were identified on DUS. Mean minimum above-knee GSV diameters were 3.8 ± 1.3 mm for CTA versus 2.9 ± 0.9 mm for DUS; mean below-knee GSV diameters were 2.6 ± 0.8 mm for CTA versus 2.5 ± 0.9 mm for DUS. Inter-observer reproducibility of CTA diameter measurements was excellent above-knee [intraclass correlation coefficient (95% CI): 0.86 (0.75-0.92)] and below-knee [intraclass correlation coefficient (95% CI): 0.77 (0.57-0.88)]. Correlation between CTA and DUS-based GSV diameters was highly significant at both above-knee (ρ=0.64, p<.0001) and below-knee (ρ=0.60, p 0.0017) locations (Figure). For identification of adequate bypass conduit using CTA, above-knee GSV diameter ≥3.9 mm was 65% sensitive and 74% specific; below- knee GSV diameter ≥3.0mm was 56% sensitive and 94% specific.
Conclusions- CTA-based GSV diameter measurements have excellent reproducibility and highly significant correlation with DUS. CTA-based GSV diameter is a specific but relatively insensitive indicator of adequate bypass conduit. When CTA-based diameters indicate inadequate GSV bypass conduit, confirmatory DUS vein mapping is warranted. Confirmatory DUS vein mapping may be unnecessary when adequate vein diameter is identified on CTA. 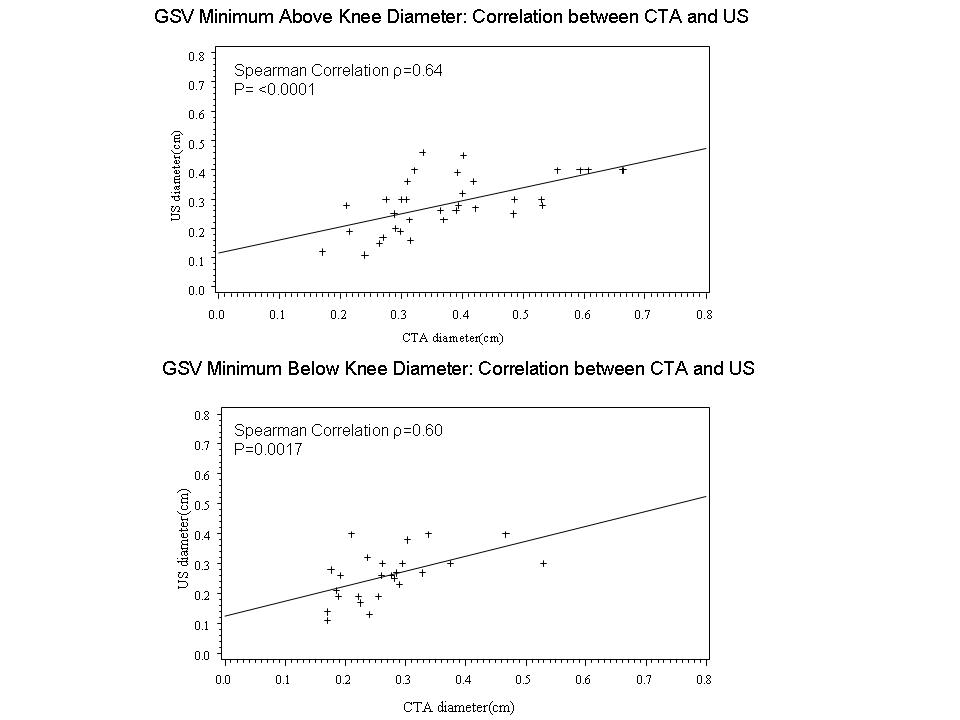
Back to Annual Meeting Program