
Back to Annual Meeting Program
Robotic thoracoscopic first rib resection and scalenectomy for treatment of Pagett-Schroetter Syndrome
Richard F Neville1, Farid Gharagozloo2, Mark Meyer3, Barbara Tempesta2, Srini Tummala4
1George Washington University, Washington, DC;2Washington Institute of Thoracic and Cardiovascular Surgery, Washington, DC;3Institute of Thoracic and Cardiovascular Surgery, Washington, DC;4Reston Radiology Consultants, Reston Hospital, Reston, VA
Objectives: First rib resection is a key component of the treatment for axillo-subclavian venous thrombosis due to thoracic outlet compression (Paget-Schroetter syndrome). Previously described techniques, transaxillary and supraclavicular, have been criticized for incomplete rib resection and neurovascular complications. We describe a minimally-invasive robotic transthoracic approach for resection of the first rib with scalenectomy.
Methods: Over a 16 month period, 13 robotic first rib resections were performed in 9 patients. Pre-operative assessment included physical exam Duplex ultrasound, and venography. All patients were tested for hypercoagulability prior to initiating anticoagulation. Based on a thoracoscopic platform, three 2 cm incisions introduced the robotic arms. The robot was used to dissect the first rib and divide the scalene muscles. The right robotic arm was replaced with a thoracoscopic 6 mm kerrison which divided the rib at its midpoint. The right robotic arm was then re-positioned with the remainder of the procedure performed robotically. Division at its midpoint allowed the rib to be pivoted on the sternal and vertebral joints. The rib was dissected from the scalene muscles and disarticulated at the respective joints. Postoperative outcomes were assessed by symptom relief, physical examination, and venography.
Results: Patient demographics included 6 men and 3 women with a mean age of 34 +/- 8 years. Coagulation studies were negative in 5 patients (56%) and positive in 4 (44%); Factor V Leiden deficiency 1, MTHFR gene mutation in 3. Operative time was 188 +/- 31 minutes. Patients were anticoagulated with warfarin for 3 months. Four patients underwent postoperative subclavian vein stent deployment after angioplasty with the addition of antiplatelet therapy. There were no perioperative complications and no mortality. At a median follow-up of 8 months, all patients had patent subclavian veins by venography and all reported being symptomatically improved.
Conclusions: Robotic transthoracic first rib resection is feasible. The technique allows for a minimally-invasive en bloc resection of the offending portion of the first rib with scalenectomy, with no neurovascular complications in this initial cohort. While greater experience is necessary, this new approach to first rib resection may allow for a minimally invasive, effective treatment for patients with Paget-Schroetter syndrome. 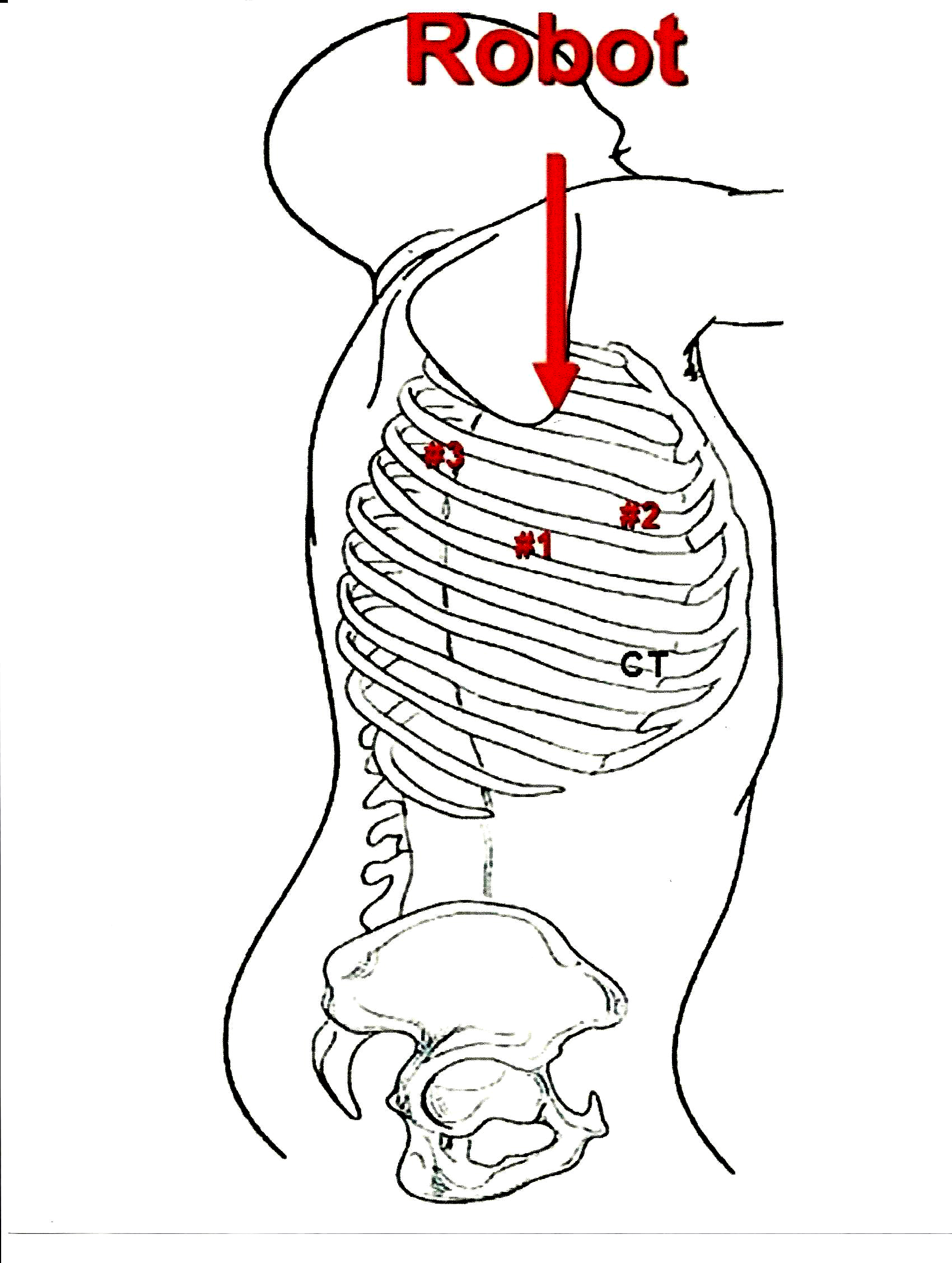
Back to Annual Meeting Program