
Back to Annual Meeting Program
Urgent Fenestrated Endovascular Aortic Aneurysm Repair (FEVAR) for a Contained Rupture of a Juxtarenal Pseudoaneurysm Secondary to Transrenal Stent Fracture
Martyn Knowles, Gregory A Stanley, M Shadman Baig, R James Valentine, Carlos H Timaran
University of Texas - Southwestern, Dallas, TX
Background: Fenestrated endovascular aneurysm repair (FEVAR) may be an alternative in patients unfit for open repair and with morphology not suitable to conventional endovascular repair. We report the case of a contained rupture of a juxtarenal pseudoaneurysm secondary to a posteriorly displaced transrenal fractured stent of a Renu device used for endovascular repair of a migrated AneuRx device.
Methods and Results: A 71-year-old male presented with a tender pulsatile abdominal mass. He had initially undergone an EVAR with an AneuRx (Medtronic, Minneapolis, MN) endograft with subsequent migration. A Zenith Renu aortouniiliac (AUI) device (Cook Medical Inc., Bloomington, IN) and femoral - femoral crossover bypass were performed 9 years later for endovascular repair of the displaced endograft (Figure 1A). Now, three years later, the patient presented with hypotension and tender, pulsatile abdominal mass. A CT angiogram revealed a contained rupture of a juxtarenal pseudoaneurysm that appeared to originate in a posteriorly displaced fracture of the transrenal stent of the Renu device (Figure 1B-D). In addition, multiple liver and lung lesions were detected concerning for malignancy. High left brachial and right percutaneous femoral access were obtained. A Cook TX2 cuff (Cook Medical Inc., Bloomington, IN) was customized with a scallop for the celiac and superior mesenteric arteries (SMA) and small fenestrations for each renal artery. The renal fenestrations were prewired to be cannulated through brachial access. Sequential endograft deployment and catheterization of the renal arteries was performed. Despite one of the renal arteries crossing through the bare stent of the Renu device, catheterization and stenting using 5mm x 22mm iCAST (Atrium, Hudson, NH) stents was performed without difficulty (Figure 2A). A converter was placed distally and carried into the iliac limb. A completion angiogram showed complete exclusion of the ruptured pseudoaneurysm and no evidence of endoleak (Figure 2B). The patient was hemodynamically stable and asymptomatic following repair with complete resolution of abdominal pain.
Conclusion: FEVAR is a useful treatment modality for urgent aortic pathology not amenable to EVAR or open repair.
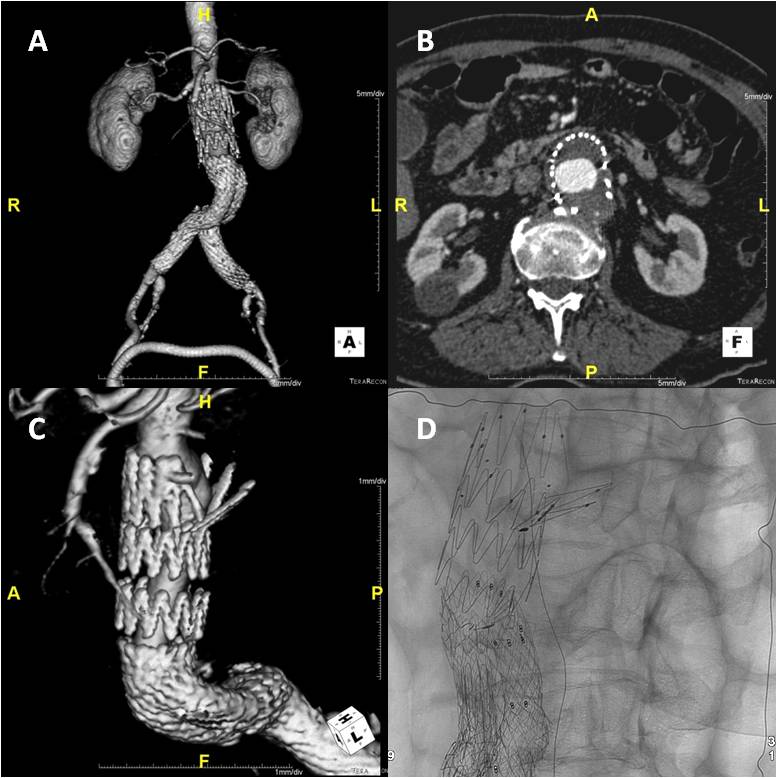
Figure 1: A: 3-D reconstruction showing the slipped AneuRx endograft with proximal Renu AUI and femoral-femoral crossover. B: Axial imaging showing a posterior contained ruptured pseudoaneurysm and stent fracture. C: 3-D imaging showing the posteriorly displaced transrenal stent fracture and associated pseudoaneurysm. D: Fluoroscopy showing strut fracture of the transrenal stent.
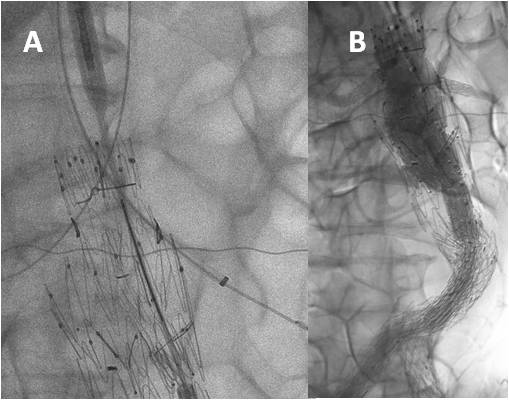
Figure 2: A: Fluoroscopy showing catheter access into the bilateral renal arteries, crossing through the transrenal stent on the left. B: Completion angiogram with successful scallop for the celiac and SMA, and bilateral renal artery stent placement.
Back to Annual Meeting Program