
Back to Annual Meeting Abstracts
Optimizing Treatment for Chronic Mesenteric Ischemia: A Comparison of Open and Endovascular Repair in a Clinical Decision Model
Wouter Hogendoorn1, MG Myriam Hunink2, Felix JV Schlosser1, Frans L Moll3, Bart E Muhs1, Bauer E Sumpio1
1Yale University, New Haven, CT;2Erasmus MC, Rotterdam, Netherlands3University Medical Center Utrecht, Utrecht, Netherlands
Objective: Chronic mesenteric ischemia (CMI) is an uncommon disease caused by stenosis or occlusion of one or more visceral arteries. Open repair (OR) has been the treatment of choice for many years, but endovascular repair (EV) has been increasingly utilized with good short-term results. Unfortunately, there is no level-1-evidence that compares these two major treatment modalities for the treatment of CMI and there are no clear guidelines on management strategies. In this study we utilized a decision analysis model to evaluate the different interventions.
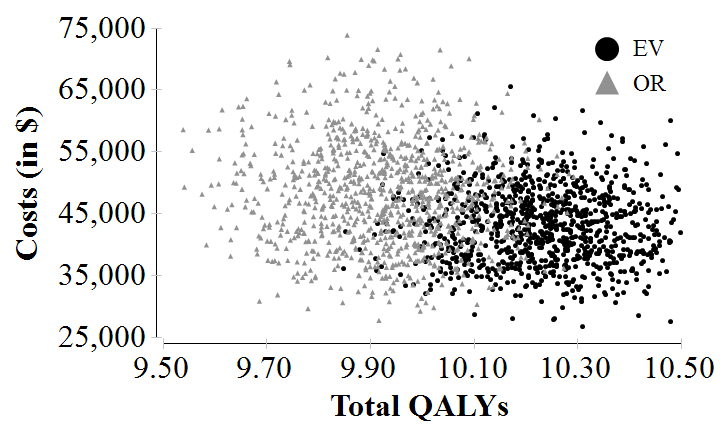
Methods: A Markov-state transition model was developed using TreeAge Pro 2012 (TreeAge Inc., Williamstown, MA) to simulate a hypothetical cohort of 10,000 65-year-old female patients with CMI requiring treatment with either OR or EV. Data and probabilities to populate the decision model, including perioperative mortality risks, complication-, reintervention-, and patency rates and disease-specific mortality, were retrieved from original and systematic reviews for CMI. Costs were retrieved using the 2013 Medicare database. Outcomes evaluated were quality-adjusted life years (QALYs), total expected lifetime costs and an incremental cost-effectiveness ratio (ICER) evaluated from the healthcare perspective. Extensive sensitivity analyses were performed for different clinical scenarios and probabilistic sensitivity analysis was performed to assess robustness of the model.
Results: For 65-year-old female patients with CMI and an average risk for operation, EV is slightly preferred with 10.24 expected QALYs (95% CI: 9.98 - 10.40) vs. 9.93 QALYs (95% CI: 9.64 - 10.19) for OR. The difference between the two strategies is comparable to 4 months in perfect health (0.31 QALYs; 95% CI: 0.06 - 0.56). Sensitivity analysis shows that the younger the patient, the greater the difference in effectiveness in favor of EV: 0.4 QALYs (at 50years) to 0.1 QALYs (at 95years). Total expected reinterventions/patient are 1.56 for EV vs. 0.28/patient in the OR group. At every age group, the number of expected reinterventions is around 5 times higher for patients initially treated with EV. Total expected costs for the reference-case patient are $48,440 ± $8,665 for OR and $43,099 ± $5,998 for EV. For patients between 50 years and 55 years old, EV is more expensive compared with OR but the ICER for EV is under the willingness-to-pay threshold of $60,000/QALY. After the age of 55, costs for OR are higher and effectiveness is lower, and therefore OR is dominated by EV.
Conclusion: The results of this decision analysis suggest that EV is slightly favored for patients with CMI. Effectiveness of EV compared with OR is always higher for every age group and risk profile. Although EV has up to five times more expected reinterventions, EV appears to be cost-effective for all patient groups. Decision analysis provides a useful means to monitor outcomes and cost-effectiveness of different treatment options. 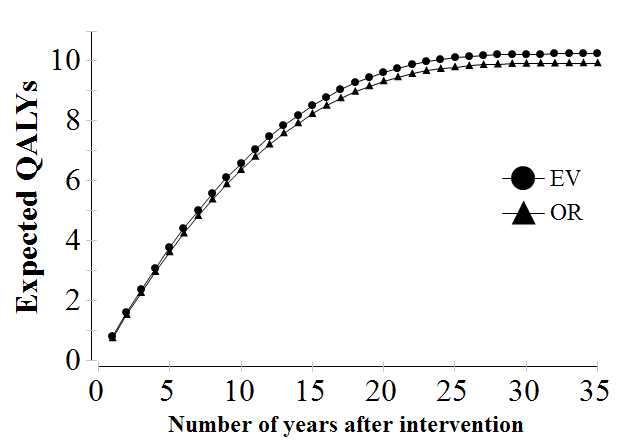
Back to Annual Meeting Abstracts