
Back to Annual Meeting Abstracts
Retrograde pedal access for patients with critical limb ischemia: Feasibility and outcomes over a three-year period
Hernan A Bazan, Linda Le, Tara Sidhom, Melissa Donovan, Taylor Smith, W Charles Sternbergh, III
Ochsner Clinic, New Orleans, LA
Background
Retrograde pedal access allows the treatment of tibial occlusive lesions when standard endovascular techniques fail. We aimed to analyze the outcomes in patients with chronic limb ischemia Rutherford class IV and V, who were otherwise not candidates for revascularization thru an antegrade access or tibial bypass.
Methods
Over a three-year period, a retrograde pedal access was selectively chosen when a popliteal or tibial lesion could not be crossed via an antegrade approach. Retrograde pedal access was performed under ultrasound-guidance using a 4-Fr micropuncture co-axial sheath. All interventions were performed in a sheathless fashion using a 0.014” or 0.018” ‘bareback’ wire as support for a 2 or 2.5 mm balloon catheter to cross and treat tibial chronic total occlusions that could not be treated via an antegrade approach. Routine anticoagulation and dual-antiplatelet therapy was used peri-procedurally. Antegrade access was used to treat any lesion that required a stent placement, after the retrograde wire was snared and brought through the antegrade guide catheter. Patient indications and comorbidities were recorded; outcomes analyzed were limb salvage rate, peri-procedural complications and mortality. Mean and standard deviations were calculated; Kaplan-Meier was used to calculate limb salvage rates.
Results
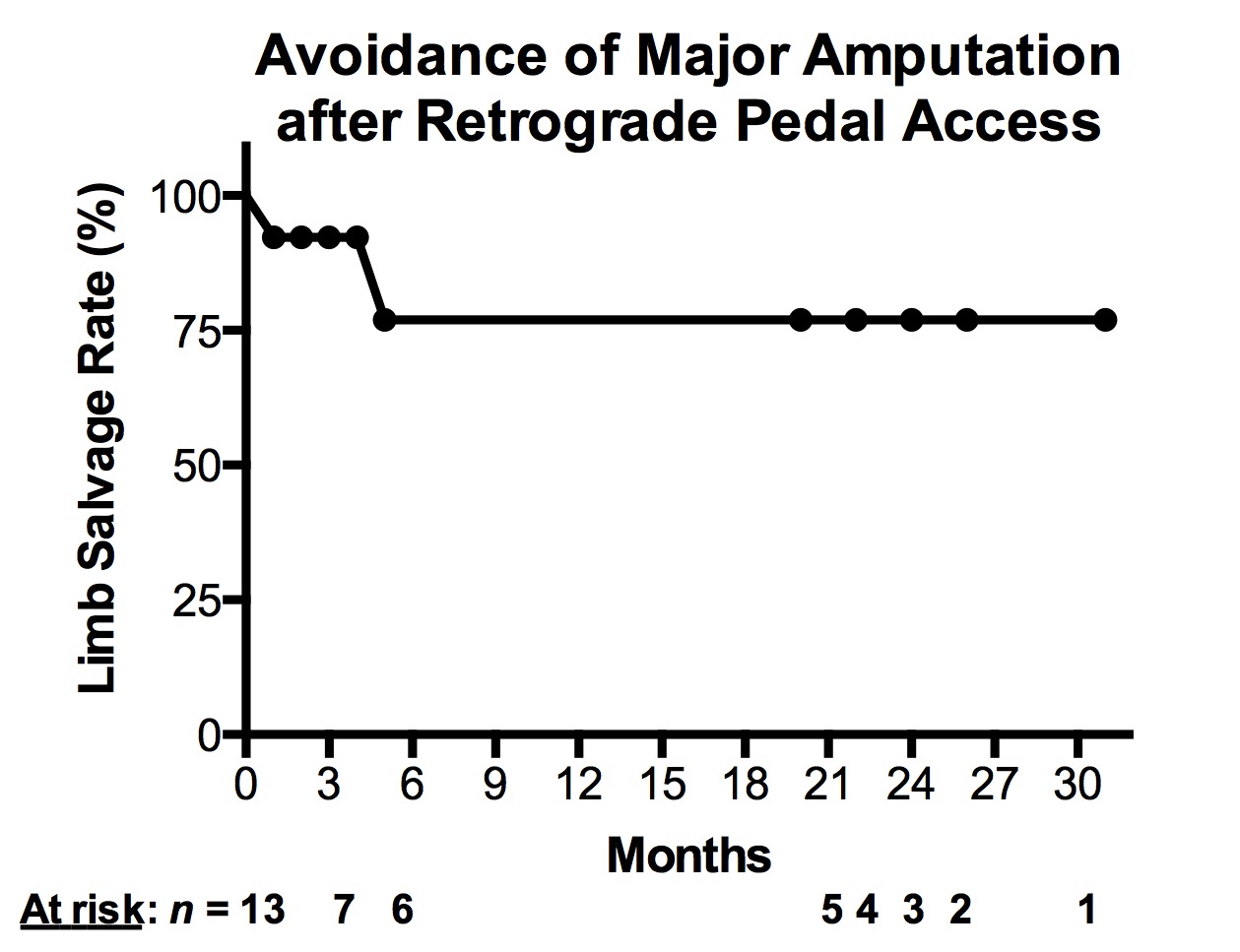
A review all lower extremity interventional angiograms from July 2010 thru August 2013 (n = 764) identified 13 cases in which a retrograde pedal access was performed (mean age was 71.4 +/- 12.4 years, 9 men). There was high prevalence of diabetes (77%; 10/13), chronic renal insufficiency (stages III - V; 69%, 9/13), and previous contralateral major amputation (38%; 5/13). Indications for a retrograde pedal revascularization were Rutherford chronic limb ischemia class IV (15%; 2/13) and class V (85%; 11/13). Technical success rate was 69% (9/13); a variety of popliteal (2/13) and tibial (13/13) vessels were intervened with angioplasty alone (10/13) via a retrograde approach and with angioplasty/stent placement (3/13). The technical failures were due to inability to cross the occlusion(s). Peri-procedurally, there was one myocardial infarction, no local complications, worsening renal insufficiency or deaths. At a mean follow-up of 13.4 +/- 10.3 months, the limb salvage rate was 77% (10/13) [Figure]. There was a high mortality rate on follow-up in this cohort (23%; 3/13) occurring at median 6 +/-4 months.
Conclusions
Retrograde pedal access for limb salvage in high-risk patients is feasible and safe with acceptable limb salvage rates at intermediate follow-up. Appropriate candidates are those who have failed an antegrade intervention and are poor candidates for a tibial bypass. Future studies should test whether this mode of revascularization has favorable limb salvage rates in larger patient populations.
Back to Annual Meeting Abstracts