
Back to Annual Meeting Abstracts
Repair of Mycotic Thoracoabdominal Aortic Aneurysm Following BCG Treatment
Kelly A Watson1, Asvin M. Ganapathi1, Matthew A. Schechter1, Brian R. Englum1, Richard L. McCann2, G. Chad Hughes1
1Division of Cardiovascular and Thoracic Surgery, Duke University Medical Center, Durham, NC;2Division of Vascular Surgery, Duke University Medical Center, Durham, NC
INTRODUCTION:
Mycobacterium bovis Bacille Calmette-Guerin (BCG) immunotherapy is a common adjuvant treatment for bladder cancer. While some side effects are mild, severe complications such as osteomyelitis and mycotic aortic aneurysm can occur. Because of the life threatening nature of these complications, better understanding of diagnosis and treatment options is essential.
METHODS:
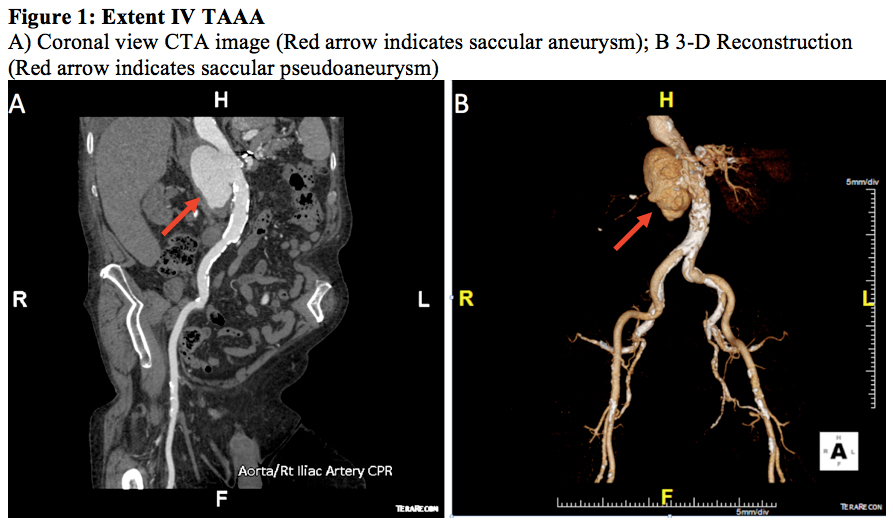
A 73 year-old Caucasian male with a history of bladder cancer treated with BCG vesicular immunotherapy presented with weight loss and back pain. Outside hospital magnetic resonance angiography study revealed a saccular Extent IV thoracoabdominal aortic aneurysm (TAAA) as well as osteomyelitis of the thoracic spine. The patient was transferred to a tertiary referral center for further management.
RESULTS:
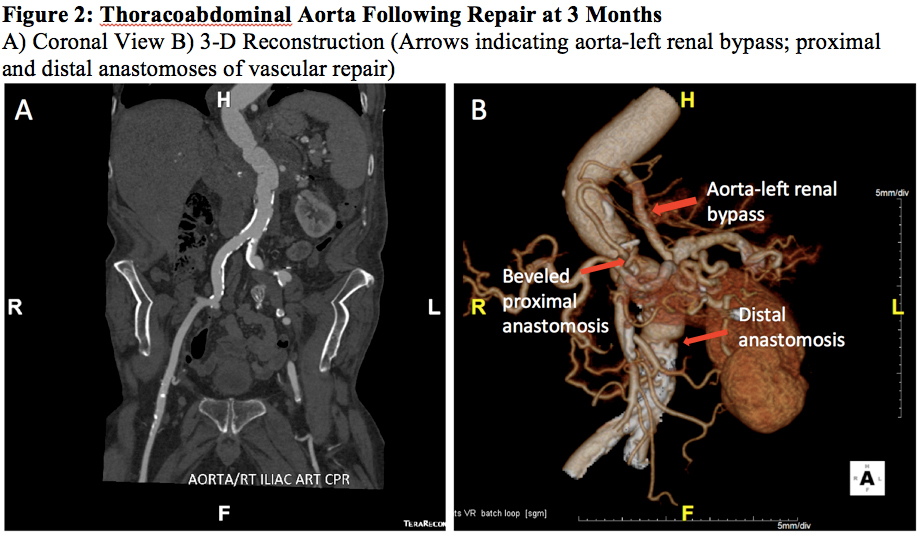
Following transfer, computed tomography angiography (CTA) confirmed the presence of a 7.2 centimeter saccular Extent IV TAAA involving the visceral segment and proximal abdominal aorta (Figure 1). After preoperative work-up, the patient underwent urgent open repair via a left thoracoabdominal approach through the 8th intercostal space. Repair was performed with initial descending thoracic aorta to left renal artery bypass with 6 mm PTFE with subsequent proximal aortic cross clamp at the level of the diaphragm just below the aorta-renal bypass, to maintain left renal perfusion during the period of aortic crossclamp. The aorta was replaced from the visceral segment, utilizing a beveled proximal anastomosis, to the mid-infrarenal aorta with a 22 mm rifampin-impregnated Dacron graft given the suspicion for mycotic aneurysm. Intraoperative findings revealed a large pseudoaneurysm which involved the visceral segment and proximal infrarenal aorta and had eroded into the spinal column. Following surgery the patient recovered uneventfully with no signs of infection. Intra-operative culture of the aneurysm wall confirmed the presence of Mycobacterium bovis necessitating a 9-month course of ethambutol, isoniazid, rifampin and pyrazinamide. Follow up at 6 months revealed no signs or symptoms of infection, and the patient continues to do well. CTA at 3 months demonstrated an intact repair with widely patent aorta-left renal bypass graft and no evidence of residual infection (Figure 2).
CONCLUSIONS:
Mycotic thoracoabdominal aortic aneurysm secondary to BCG treatment for bladder cancer is a rare, but serious complication. Awareness of potential mycotic aneurysm is important, particularly in patients presenting with constitutional symptoms and abdominal pain following BCG treatment. Given the associated inflammation, there is a high risk of rupture, necessitating prompt diagnosis and treatment. The infectious component must also be considered, and a multidisciplinary team including surgery and infectious disease specialists is essential for repair and prevention of recurrent infection. To our knowledge, this represents the first reported case of repair of a mycotic TAAA following BCG therapy and demonstrates that with prompt diagnosis, treatment, and appropriate antibiotic coverage, good outcomes can be achieved.
Back to Annual Meeting Abstracts