
Back to Annual Meeting Abstracts
Branched Endograft Repair of an Aortic Stump Aneurysm
W A Lee1, Irfan R. Imami2
1Lynn Heart and Vascular Institute, Boca Raton, FL;2TEPAS Healthcare, Melbourne, FL
INTRODUCTION: 75 yo man had an open AAA repair 10 years ago complicated 4 years later by an aortoenteric fistula. This was treated with graft excision, oversewing of the aortic stump, bilateral axillofemoral bypasses and a right AKA. A year later these became infected with multidrug-resistant Pseudomonas resulting in axillary and femoral mycotic pseudoaneurysms, which required bilateral graft excisions and a left AKA. In 2010, he underwent a thoraco-visceral/renal bypass using a rifampin-coated bifurcated graft for ischemia. Surveillance CT 2 years later showed a 5.3 cm aortic stump aneurysm. Follow-up CT a year later showed marked increase in aneurysm size to 7.0 cm. The patient remained asymptomatic without any constitutional signs, lived at home with his spouse, performed all ADLs independently, and drove in a specialized handicap vehicle.
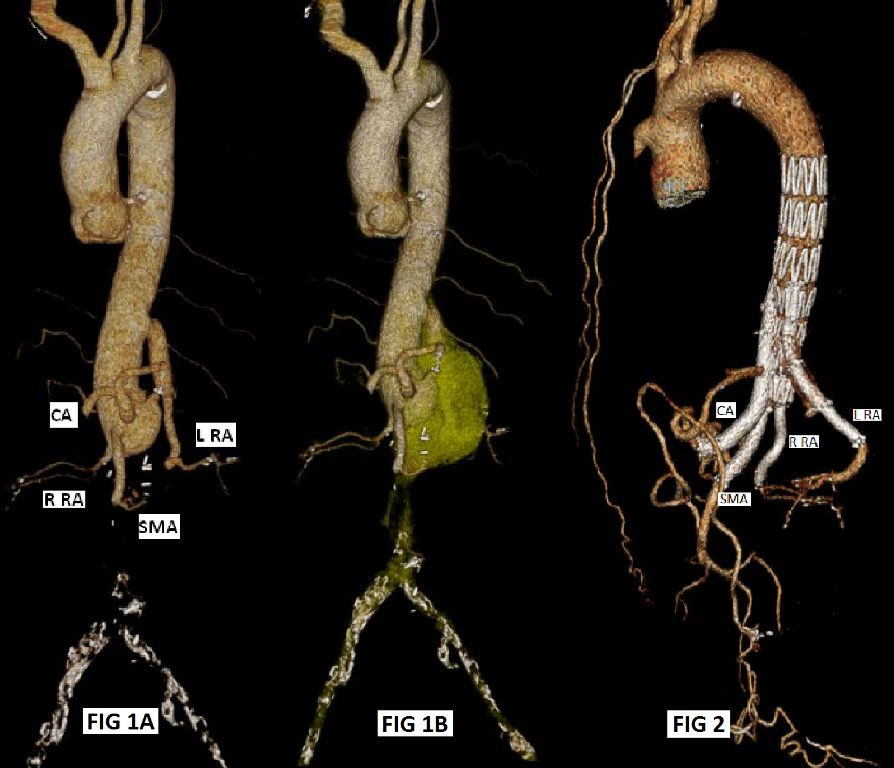
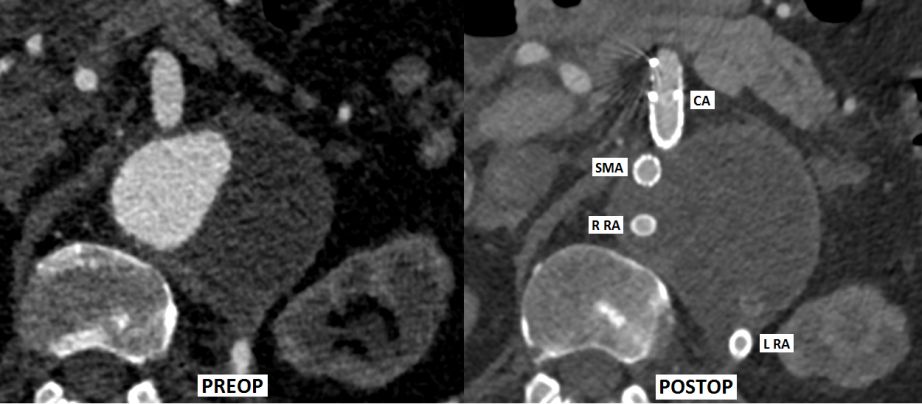
METHODS: CTA showed an aortic stump aneurysm involving the origins of the celiac, SMA and right renal arteries. A bifurcated graft originated from the distal descending thoracic aorta with one patent limb to the left renal artery and the other limb thrombosed. There was no stranding, mural thickening or other inflammatory signs.
An endovascular repair was planned using a custom-manufactured, modified Zenith t-Branch device. The device differed from the "standard" t-Branch in terms of the location of the 4-branches and the delivery system, to accommodate for the unusually proximal origin of the left renal artery graft and lack of iliofemoral access to the aorta.
The procedure was performed in 2 stages. Through a hemi-sternotomy, a 10-mm ascending aortic conduit was used for antegrade delivery of the modified t-Branch to the distal descending thoracic aorta. Afterwards, the conduit was oversewn and the sternotomy closed over chest tubes. The next day the branch portion of the repair was performed. The proximal left brachial artery was exposed and used to connect each of the 4 branches to its corresponding native visceral/renal artery using a combination of covered and uncovered stents. The distal end of the modified t-Branch was occluded using an Amplatzer plug.
RESULTS: The procedure and fluoroscopic times for stages I/II were 187/177 min and 16/48 min, respectively. Total length of stay was 6 (incl 3 ICU) days. Pre- and postoperative renal function (Cr/eGFR) remained unchanged (1.1/>60, 1.0/>60, respectively). Patient was readmitted on POD 15 for shortness of breath. There were no neurologic events. 1-month CTA showed all 4 branches patent and complete exclusion of the aneurysm without endoleak. (Figures)
CONCLUSIONS: A modified Zenith t-Branch device was able to successfully exclude an unusual aortic stump aneurysm in a patient without surgical options. The long term durability of this type of repair in the setting of possible underlying mycotic etiology remains to be determined.
Back to Annual Meeting Abstracts