
Back to Annual Meeting Abstracts
Novel Transcatheter Angiovac utilization and endovascular stent graft placement for the treatment of symptomatic primary thoracoabdominal mural and floating intra-aortic thrombus
Joseph H Habib, James Cunningham, Kristy Cosgrove
University of Florida, Jacksonville, FL
INTRODUCTION:
Primary aortic mural thrombus in a non-aneurysmal non-atherosclerotic aorta is an uncommon clinical finding. Catastrophic embolic complications may occur if the thrombus is mobile. Patient presentation is variable and can include arterial thromboembolism with potential of visceral and peripheral involvement.
Management of spontaneous aortic mural thrombus has remained poorly defined. Therapeutic options include anticoagulation, thrombolysis, balloon catheter thrombectomy, aortic replacement, and endovascular exclusion. Anticoagulation alone can result in a high rate of continued embolization while high morbidity and mortality rates may accompany open surgical options such as thoracoabdominal aortic replacement.
The AngioVac system (Angiodynamics, Latham, NY) is intended for use as a venous drainage cannula for removal of venous or tumor thrombus from the ileocaval system and right heart chambers during extracorporeal bypass. The device is inserted through a cannula into the venous system. A return cannula is placed into the venous system to complete the circuit. The cannulas are connected to an extracorporeal pump and negative pressure is generated up to 80mmHg. The negative pressure functions to remove the intravascular debris in an en-bloc fashion. The circuit includes a filter to trap the debris before re-infusing the blood.
The use of AngioVac in the treatment of thrombus in the arterial system has yet to be described. We present the first case report of successful treatment of symptomatic thoracoabdominal mural and floating intra-aortic thrombus using a thoracic endograft (C-TAG, W. L. Gore and Assoc., Flagstaff, AZ) in conjunction with the AngioVac device.
METHODS:
A 46-year-old female presented with primary aortic mural thrombus beginning mid descending aorta with extension distally into the celiac artery and evidence of visceral embolization demonstrated on CTA (Fig 1).
The patient was taken to the angiography suite for exclusion of the aortic thrombus with an endograft in conjunction with percutaneous celiac thrombectomy.
Follow-up CTA revealed thrombus extending from beneath the distal landing zone of the endograft into the abdominal aorta which appeared to be floating in the visceral segment.
The patient was brought back to the angiography suite for AngioVac thrombectomy. Bilateral femoral cutdowns were performed and the Angiovac device was placed through the iliofemoral arterial system into the abdominal aorta with the return venous cannula placed in the contralateral femoral vein.
RESULTS:
Successful extraction of the thrombus was achieved and confirmed on follow-up CTA imaging (Fig 2).
CONCLUSIONS:
This case demonstrates the effective utilization of an endograft and AngioVac thrombectomy as an effective treatment option for select patients with symptomatic primary thoracoabdominal aortic mural thrombus. Ease of use and low risk profile suggests this technique could become a front line option for select patients. Long term follow up will be necessary to assess durability of this technique.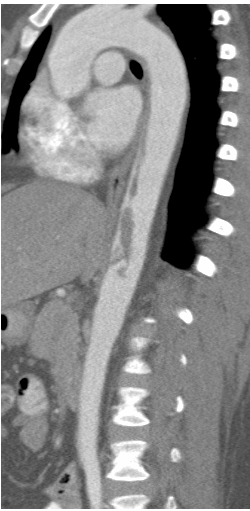

Back to Annual Meeting Abstracts