
Back to Annual Meeting Posters
Ultrasonic accelerated thrombolysis of IVC thrombosis
Mark E O'Donnell, Sailendra G Naidu, Ryan Day, Grant T Fankhauser, William M Stone, Richard J Fowl, Fadi E Shamoun, Samuel R Money
Mayo Clinic, Phoenix, AZ
INTRODUCTION: Inferior vena cava (IVC) thrombosis remains rare with an incidence of 0.4% in some venous thromboembolism series. Successful ultrasonic accelerated thrombolysis, using the EkoSonic Endovascular System (EKOS® Corporation, Bothell, WA), has been previously reported in patients with iliac vein and lower extremity deep venous thrombosis (DVT). We describe our initial experience with ultrasonic accelerated thrombolysis of IVC thrombosis.
METHODS:All patients diagnosed with symptomatic IVC thrombosis who were treated with ultrasonic accelerated thrombolysis from January 2012 to August 2013 were included for review. Patient data regarding clinical presentation, thromboembolic risk factors, pertinent imaging, treatment pathway and clinical outcome were recorded.
RESULTS: Seven patients (5 males, 2 females, mean age 58.1 years) presented with lower extremity DVT. Four patients had a history of neoplastic disease and two were current smokers. Four patients had a history of previous DVT and 6 patients a history of pulmonary emboli. All seven patients were previously anticoagulated and had IVC filters in-situ. Pro-thrombotic hematological analyses were negative for all patients. Ultrasound duplex imaging identified proximal lower extremity thrombus in four patients (57%) while cross-sectional imaging confirmed thrombus extending from the iliac veins into the IVC in all seven patients. All patients were initially treated with limb elevation, compression hosiery combined with intravenous therapeutic unfractionated heparin infusions. The indication for thrombolytic therapy was continued significant symptomatology in all patients. Following venography and confirmation of clot burden in the IVC, the thrombus was crossed and bilateral EKOS catheters were placed extending into the suprarenal IVC. EkoSonic treatment was commenced with combined infusions of 0.5mg tissue plasminogen activator and 35mls of normal saline coolant via the EKOS catheters and 500IU of heparin via the 7-Fr sheath per hour to each limb separately. After twenty-four hours, repeat venography was satisfactory in one patient. The remaining six patients required mechanical thrombectomy using the Angiojet® system (Possis Medical, Minneapolis, MN), and balloon angioplasty if necessary, which resulted in satisfactory flow in five patients (Figure 1). The remaining patient required an additional twenty-four hour EKOS infusion followed by further mechanical thrombectomy before satisfactory flow was obtained. All patients are currently well and remain anticoagulated (warfarin=6, rivaroxaban=1) with improvement in lower extremity symptomatology and no recurrence of IVC thrombosis (mean follow-up 7.6, range 1-20 months).
CONCLUSIONS: This is the first reported series of ultrasonic accelerated thrombolysis for IVC thrombosis. These early results suggest this modality may be helpful in treating patients with large IVC thrombus burden and significant clinical symptoms with successful clot dissolution and satisfactory venous flow without significant patient distress or complications.
FIGURE 1:Venography demonstrating poor bilateral flow via iliac veins into IVC (A). After 24-hours of ultrasonic accelerated thrombolysis, flow via the left common iliac vein was still not satisfactory (B). Mechanical thrombectomy and balloon angioplasty were performed. Final venogram demonstrating satisfactory flow through both iliac veins into IVC (C). 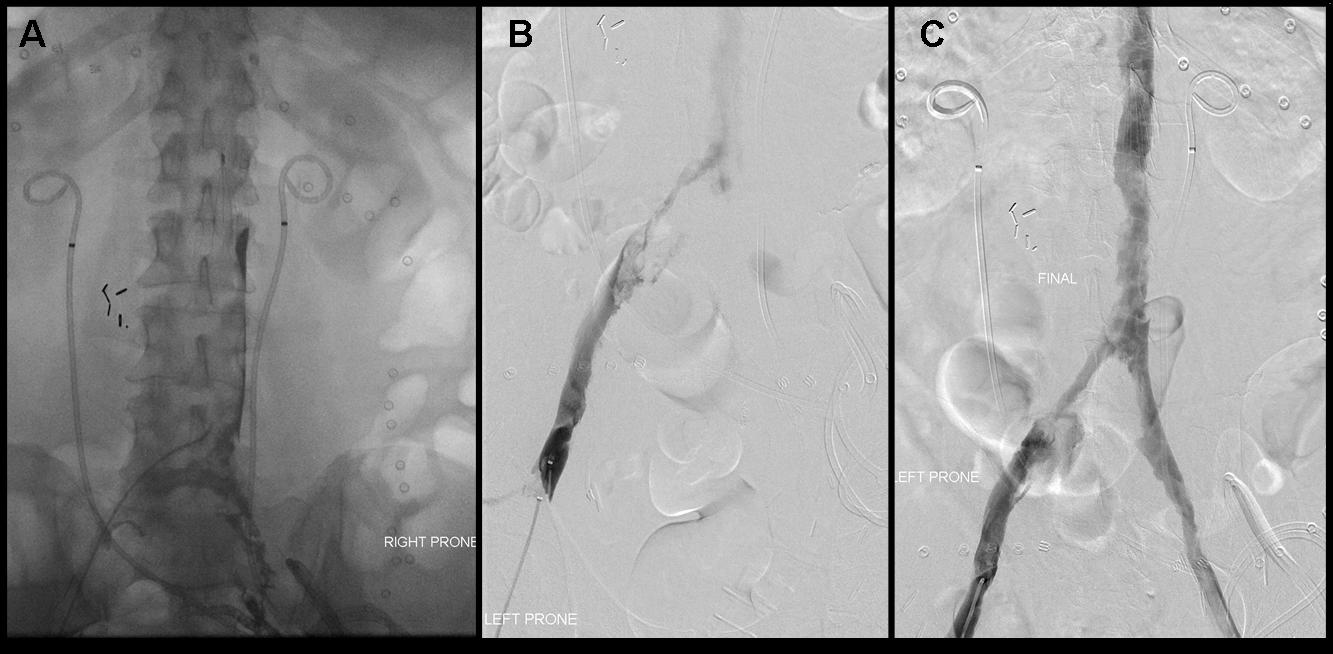
Back to Annual Meeting Posters