
Back to 2015 Annual Meeting Abstracts
Antiplatelet and statin treatment is not associated with reduced myocardial infarction after high risk vascular procedures
Randall R DeMartino1, Andrew W Hoel2, Adam W Beck3, John W Hallett4, Shipra Arya5, Gilbert H Upchurch6, Jack L Cronenwett7, Philip P Goodney7
1Mayo Clinic, Rochester, MN;2Norwestern University Feinberg School of Medicine, Chicago, IL;3University of Florida, Gainesville, FL;4Roper St Francis, Charleston, SC;5Emory University, Atlanta, GA;6University of Virginia, Charlottesville, MN;7Dartmouth-Hitchcock Medical Center, Lebanon, NH
Objective: Medical management (MM) with antiplatelet (AP) and statin therapy is recommended for most patients undergoing vascular surgery. We evaluated the pre-operative use of these on post-operative myocardial infarction (MI) in patients undergoing high-risk procedures within the Vascular Quality Initiative (VQI).
Methods: We studied VQI patients undergoing elective supra- (3,039) and infra-inguinal bypass (n=8,323) and open AAA repair (n=3,007) from 2005-2014. We examined the use of MM (AP and/or statin) on post-operative MI and post-operative death. Multivariable analyses were performed to identify factors associated with pre-operative MM use as well as and MI and MI/death rates across procedures and cardiac risk strata (utilizing VSGNE cardiac risk criteria).
Results: Overall, most patients were on both AP and statin at the time of surgery (56% vs. 12% neither agent, 19% AP only, 17% statin only) and MM was similar across procedure groups. Rates of MI were similar despite MM strategy, with slightly higher rates in patients on both agents (neither AP or statin 2.4%, AP only 2.6%, statin only 2.8%, both 3.7%, p=0.003). MI increased with cardiac risk (1.8% vs 3.8% vs 6.5% for low, medium and high risk, p<0.01). When MI was stratified by cardiac risk, MM did not reduce MI rates, and was slightly higher for patients on both agents (Figure). After multivariable adjustment for MI, MM was not associated with reduced MI compared to those on neither medication (AP only: OR 1.0 95% CI 0.6-1.5, Statin only: OR 0.9 95% CI 0.5-1,4, Both agents: OR 1.0 95% CI 0.7-1.5, p>0.05 for all). Findings were similar for combined outcome of MI/death. Finally, analysis demonstrated that APs and statins were used more often in patients with known cardiovascular risk factors.
Conclusions: These data confirm that MI events are highly associated with a patient’s estimated cardiac risk. However, lack of MM did not result in higher rates of MI. It appears that higher risk patients are currently selected for MM in VQI, but that this is not associated with reduced post-operative MI or MI related mortality.
Figure – Rates of MI by treatment with antiplatelet and statin medications across cardiac risk.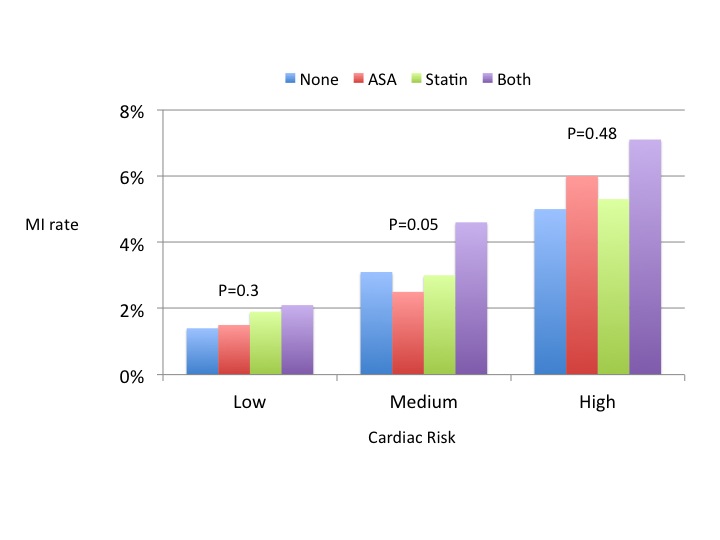
Back to 2015 Annual Meeting Abstracts