
Back to 2015 Annual Meeting Abstracts
Current Accepted Hemodynamic Criteria For Critical Limb Ischemia (CLI) Do Not Accurately Stratify Patients At High Risk For Limb Loss
Raghuveer Vallabhaneni, Corey A. Kalbaugh, Ana Kouri, Mark A. Farber, William A. Marston
University of North Carolina-Chapel Hill, Chapel Hill, NC
Introduction:
Critical limb ischemia has been defined as patients with rest pain or tissue loss who have an ankle pressure(AP) < 70 mm Hg or toe pressure (TP)< 50 mm Hg. Data suggesting these patients are at high risk for limb loss without successful revascularization is limited. This study was designed to identify limb loss and mortality rates in patients who did not respond to revascularization or who were not revascularized and to determine whether CLI hemodynamic criteria accurately identify patients at high risk for limb loss.
Methods:
Between 2008 and 2010 all patients undergoing lower extremity arterial duplex testing at our hospital were identified. Those with AP below 70 or TP below 50 were retrospectively reviewed to determine whether they had symptoms of rest pain or tissue loss qualifying them for analysis in the database. Patients who underwent revascularization and subsequently had post-revascularization AP or TP greater than the CLI criteria were removed from the cohort. Demographic factors, wound healing, amputation rates and mortality were obtained and analyzed in relation to the initial ankle and toe pressures. Outcomes were measured using Kaplan-Meier life table analysis and Cox proportional hazards models.
Results:
Three hundred eighty-one patients presented with 443 limbs identified meeting CLI criteria. After revascularization, 98 limbs with AP and/or TP improved to greater than 70 and 50 mm Hg were removed from the study cohort. In 45 limbs, patients did not respond to intial revascularization and their AP and/or TP remained within CLI criteria. These limbs remained in the patient cohort yielding a final group of 296 patients and 345 limbs. Mean follow-up time was 2.0 years. In the entire patient cohort, limb loss occurred in 24% at 1 year and in 31% at 3 years. Mortality was 32% at 1 year and 56% at 3 years. Amputation-free survival was 54% at 1 year and 28% at 3 years. Lower toe pressures were associated with a significantly higher incidence of amputation. Among those with an initial toe pressure ≤10 mm Hg (n=85), limb loss occurred in 46 % at 1 year and 60% at 3 years. This limb loss was significantly greater than limb loss among those with a toe pressure 31-50 mm Hg (n=115, 18% at 3 years, p<.001, Figure). Amputation free survival in patients with a toe pressure ≤ 10 mm Hg was 8% at 3 years.
Conclusions:
CLI is associated with a high mortality, but not all patients with currently defined hemodynamic criteria for CLI are at high risk of limb loss. Patients with a toe pressure between 31 and 50 mm Hg (41% of the cohort) and not receiving revascularization or not responding hemodynamically to revascularization experienced a low risk of limb loss. We recommend revising the hemodynamic criteria for CLI to better identify patients at high risk for limb loss who require intervention to improve outcomes.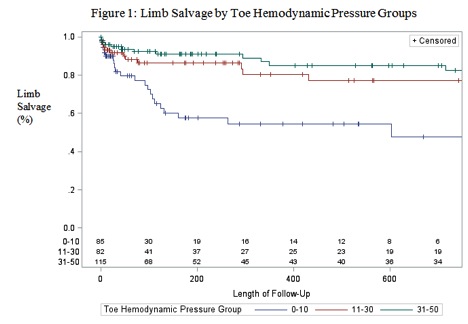
Back to 2015 Annual Meeting Abstracts