
Implications of Secondary Aortic Intervention after TEVAR for Acute and Chronic Type B Dissection
Salvatore T. Scali1, Kristina A. Giles1, Salim Lala1, Suzannah Patterson1, Martin Back1, Javairiah Fatima1, Dean Arnaoutakis1, Scott A. Berceli1, Thomas S. Huber1, Adam W. Beck2
1university of florida- gainesville, Gainesville, FL;2University of Alabama-Birmingham, Birmingham, AL
INTRODUCTION: Thoracic endovascular aortic repair(TEVAR) has become the mainstay of treatment for acute, complicated type B dissection(TBAD). Similarly, TEVAR has been increasingly used to manage chronic TBAD with aneurysmal degeneration. Dynamic aortic morphology with TBAD may have significant consequences on TEVAR durability. However, few descriptions contrast the differences in secondary aortic intervention(SAI) after TEVAR for acute(AD)/chronic(CD) TBAD. The purpose of this analysis is to examine the incidence, timing, and types of SAI after TEVAR for acute/chronic TBAD and describe SAI impact on survival.
METHODS: A single center retrospective review was performed on all TEVARs for acute/chronic TBAD from 2005-2016. Patients with staged(<30-days) or concomitant ascending aortic repair/arch replacement were excluded. Acuity was defined as symptom onset within 0-30 days(AD) or >30-days(CD). SAI procedures were grouped into open(intended treatment zone or remote aortic site), major endovascular(TEVAR extension or endograft implanted at non-contiguous aortic site) or minor endovascular(side-branch or false lumen embolization) categories. Kaplan-Meier methodology was used to estimate freedom from SAI and survival. Cox proportional hazard modeling was used to identify predictors of SAI.
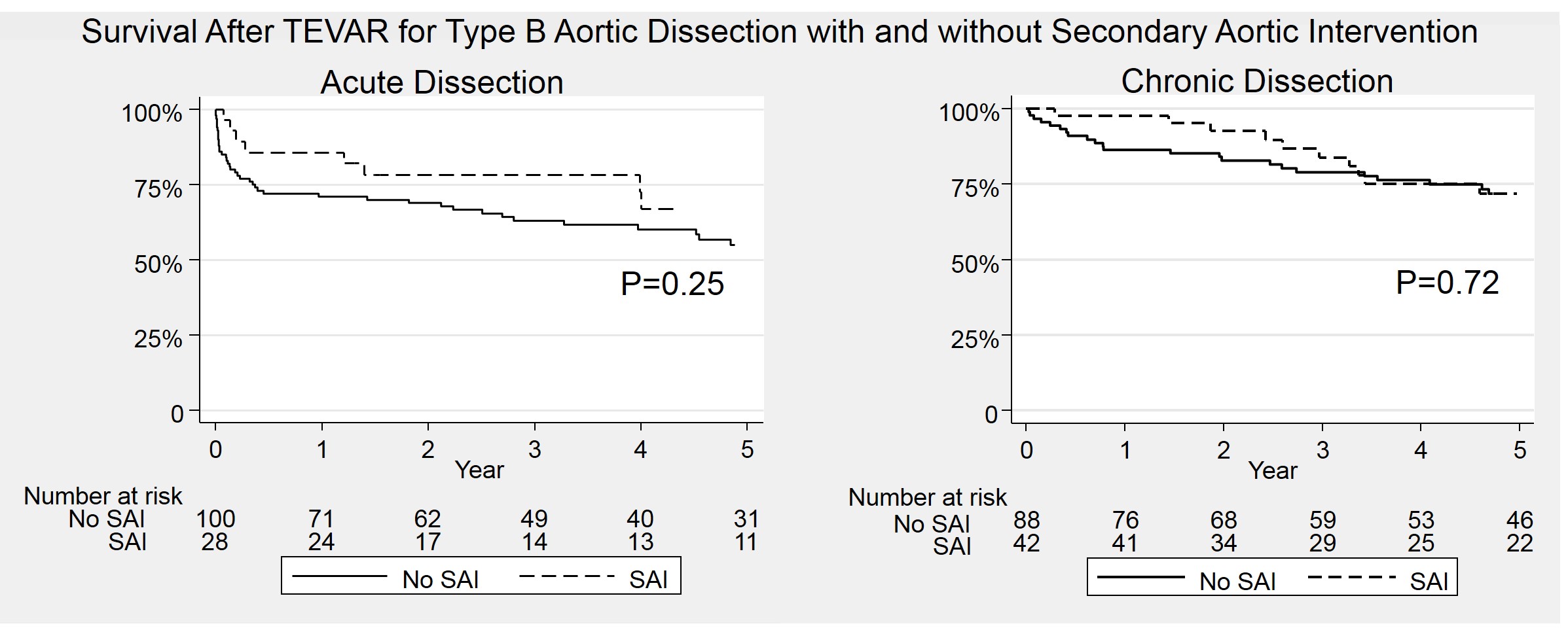
RESULTS: A total of 258 patients underwent TEVAR for acute[AD, 49%(n=128)] and chronic[CD, 51%(n=130)] TBAD. Overall, mean follow-up was 17±22 months with an SAI rate of 27%[n=70; AD, 22%(28) vs. CD, 32%(42);CD OR 1.7, 95%CI 0.9-2.9;p=.07]. Median time to SAI was significantly less for AD(0.7[0-12)] vs. CD, 7[0-91]months;p<.001). However, freedom from SAI was similar(1-year:AD, 67±4% vs. CD, 68±5%;3-year: AD, 65±7% vs. CD, 52±8%;p=.71)(Figure 1). Among SAIs, re-intervention type was similar for AD and CD patients(open, 61% vs. 55%;p=.62;major endovascular, 36% vs. 38%;p=.84;minor endovascular, 21% vs. 21%;p=1). Overall, open conversion rate(either partial or total endograft explant)[AD, 10%(13 of 128) vs. CD, 15%(20 of 130);p=.22] and retrograde dissection incidence resulting in SAI[AD, 6% vs. CD, 4%;p=.53] was similar. There was no significant difference in survival for SAI patients(5-year: AD+SAI, 55±9% vs. AD without SAI, 67±8%;p=.25; 5-year: CD+SAI, 72±6% vs. CD without SAI, 72±7%;p=.72)(Figure 2). Factors associated with SAI included younger age, AD with larger maximal aortic diameter, Marfan syndrome, and a brachiocephalic adjunctive procedure performed with index TEVAR. Indication for index procedure(aneurysm, malperfusion, rupture, or pain) or history of proximal aortic procedure were not predictive of SIA.
CONCLUSIONS: SAI after TEVAR for TBAD is common. AD has a higher proportion of early SAI, however CD patients appear to have on-going risk of remediation after the first year. The types of SAI are similar between groups and the occurrence of aorta related re-intervention does not impact survival. Patient related and procedure-specific anatomic factors influence rate of SAI. These data should be taken into consideration for patient selection, device design and surveillance strategies after TEVAR for TBAD. 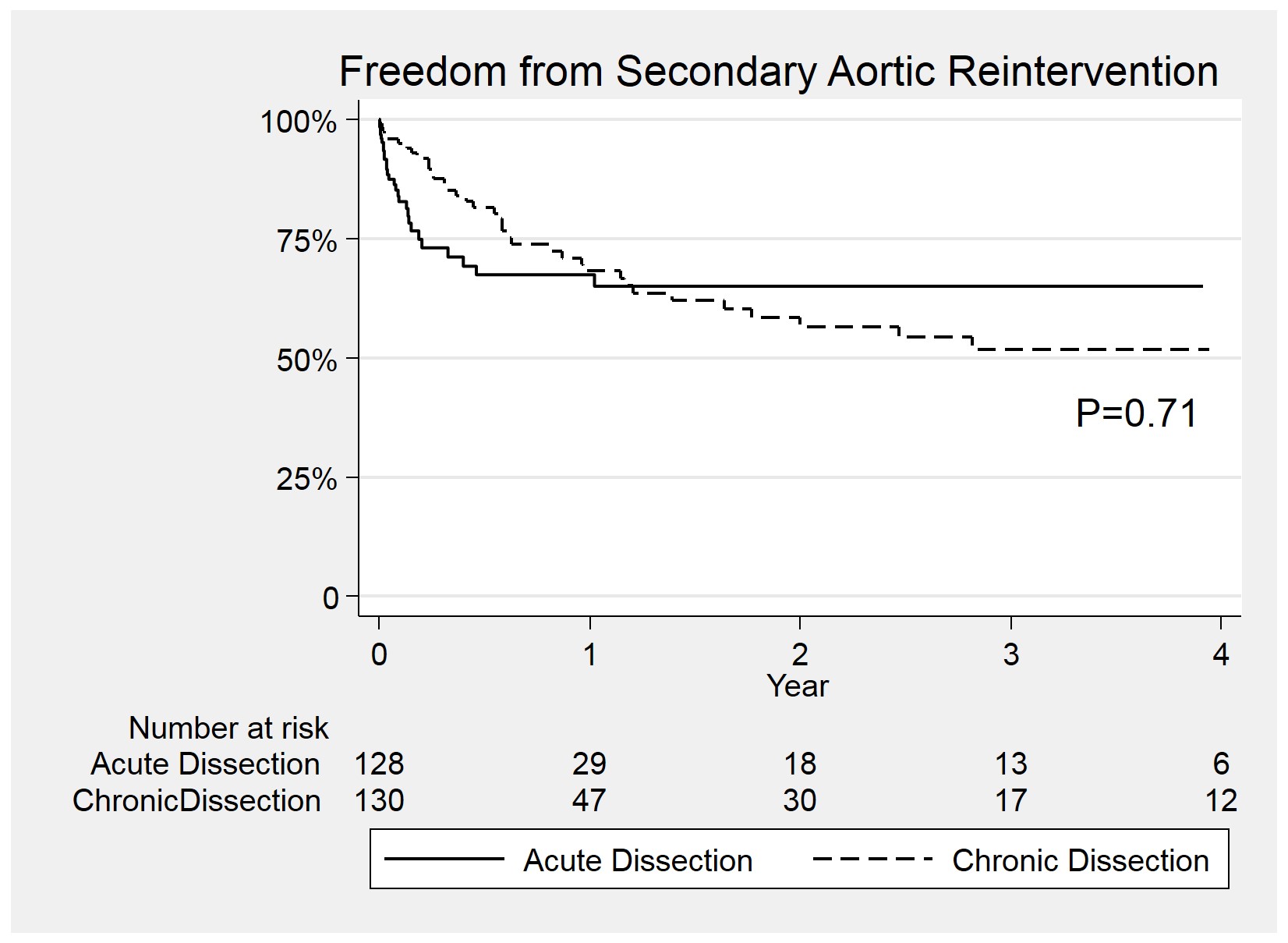
Back to 2018 Abstracts



