
Rotational Vertebral Artery Occlusion Caused by Completely Extra-osseous Vertebral Artery
Kristyn A Mannoia, Steven Reiman, William P Shutze, Sr.
The Heart Hospital Baylor Plano, Plano, TX
INTRODUCTION: Rotational vertebral artery occlusion (RVAO) can occur at the V4 segment (Bowhunter's syndrome) or in the V2 segment of the vertebral artery (VA). In the latter situation this is usually due to compression from the longus colli tendon or cervical osteophytes. We present a case of RVAO in a patient with a completely extraosseus course of the V2 segment of her dominant right VA. CASE PRESENTATION: A 76 year old female presented with the recent onset of drop attacks reproducibly precipitated by turning her head to the right. A CT angiogram demonstrated hypoplastic left VA and a completely extraosseus V2 segment of the right VA. The CTA was repeated with her head turned moderately to the right and demonstrated narrowing of the right VA caused by extrinsic compression from the thyroid cartilage. She underwent arteriolysis of the V2 segment of the VA with release of restrictive bands of the levator scapulae as well as resection of the posterior superior thyroid cartilage. Intraoperative duplex ultrasonography did not demonstrate any endoluminal fibrosis or stenosis in the VA. Rightward head rotation no longer produced VA compression. The patient’s symptoms were resolved postoperatively and she was discharged neurologically intact without swallowing difficulties on postoperative day 1. A followup CT scan with head rotated showed no sign of VA compression. DISCUSSION: This is a novel case of a completely extraosseus V2 vertebral artery with rotationally induced compression producing symptomatic vertebrobasilar insufficiency. This unusual anatomic variant has not previously been reported. The unprotected and unrestricted positioning of the V2 segment allowed this portion of the VA to become redundant, predisposing it to compression by the levator scapulae and the adjacent segment of the thyroid cartilage. Arteriolysis and resection of the impinging portion of thyroid cartilage resulted in resolution of the RVAO. CONCLUSIONS: When evaluating patients for RVAO vascular surgeons should be aware of this anatomic variant as a potential etiology. Surgical correction with arteriolysis and resection of the adjacent compressive structures results in symptomatic relief. 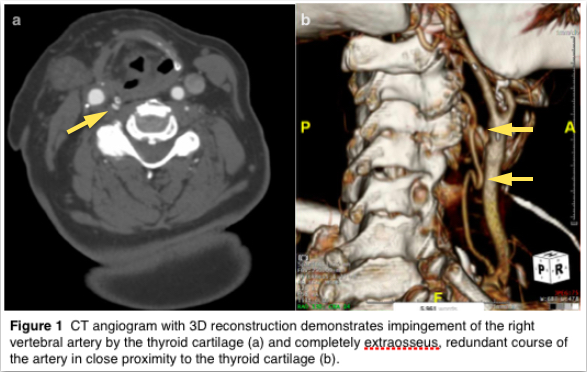
Back to 2018 Abstracts



