
TEVAR for Descending Thoracic Aortic Aneurysm with Double Aortic Arch
Bruce Tjaden, Jr., Maria Codreanu, Ali Azizzadeh
The University of Texas Health Science Center at Houston, Houston, TX
INTRODUCTION: Double aortic arch (DAA) is a rare congenital anomaly that typically presents early in life with aerodigestive tract compression. Co-occurrence of descending thoracic aortic aneurysm (DTAA) and DAA has not been previously reported. We present a case of endovascular management of a patient with both pathologies.
METHODS: An 83 year-old Chinese man underwent computed tomography scan after a fall. Incidental note was made of a complete double aortic arch (DAA) producing a vascular ring encircling the trachea and esophagus, and a 5.5cm descending thoracic aortic aneurysm (DTAA) (Fig. 1). The right arch gave rise to the right subclavian and right common carotid arteries, while the left arch gave rise to the left common carotid and left subclavian arteries. The arches fused at a point distal to the left subclavian artery. The patient had sustained multiple rib fractures and other injuries during his fall, and due to his need for prolonged respiratory support and serial orthopedic procedures, vascular surgery was deferred at the time of diagnosis. During surveillance over the subsequent two years, his aneurysm grew to 6.3cm in size, and he began to have left chest pain. The patient was offered endovascular repair using a commercially available device. The procedure was performed in a hybrid operating room under general anesthesia with cerebrospinal fluid drainage. Diagnostic angiography performed via a right femoral approach confirmed appropriate landing zones for stent-graft placement. After pre-deploying two Proglide Perclose devices (Abbott, IL) in the left femoral artery, a 34mmx20cm Conformable Thoracic Aortic Graft device (cTAG) (WL Gore, AZ) was positioned and deployed distal to the convergence of the two aortic arches. This excluded the entirety of the DTAA. (Fig. 2).
RESULTS: The patient’s postoperative course was unremarkable, and he was discharged in good condition.
CONCLUSIONS: During development, failure of involution of the right dorsal aorta produces a DAA, in which a right arch gives rise to the right-sided great vessels before wrapping behind the trachea and esophagus to rejoin the left arch. This anomaly is rare, but is the most common vascular ring. In most cases, the right arch is dominant, and the left arch is hypoplastic or obliterated. Co-dominance of bilateral arches is rare, occurring in only about 5% of cases. The co-occurrence of DTAA and DAA has not been reported before. DAA may complicate an endovascular approach to DTAA, as the point of fusion of the two arches could preclude adequate seal, and might mandate parallel grafting or other adjunctive techniques. In the case presented here, favorable anatomy and an asymptomatic vascular ring allowed for a relatively straightforward endovascular repair in a patient unfit for open surgery with an excellent outcome.
Figure 1
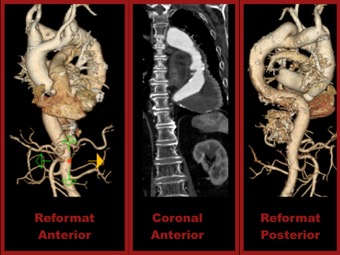
Figure 2

Back to 2018 Abstracts



