
Robotic assisted Iliofemoral Arterial Bypass for the treatment of Iliac Artery Endofibrosis
Anthony H Chau, Richard J Fowl, Erik P Castle, Victor J Davila
Mayo Clinic Arizona, Phoenix, AZ
INTRODUCTION: External iliac artery endofibrosis is a rare non-atherosclerotic occlusive vascular disease caused by chronic arterial wall stress and progressive luminal fibrosis that primarily afflicts endurance athletes. Endovascular therapy has limited role in managing endofibrosis. Open surgical reconstruction is the treatment of choice. Surgical options include long segment vein patch angioplasty, resection with autologous vein interposition, and ilio-femoral bypass grafting. We present a patient with an external iliac artery occlusion who was successfully treated by robotic assisted ilio-femoral bypass graft.
METHODS: A 55 year old female fitness instructor was referred for a vascular surgical evaluation for exertional right lower extremity pain for one year. This pain is exacerbated by bicycling and running. Her symptoms are primarily severe thigh and calf pain and foot numbness. A CT angiogram revealed an isolated complete occlusion of her right external iliac artery. Given her lifestyle and career limiting symptoms, surgical therapy was offered.
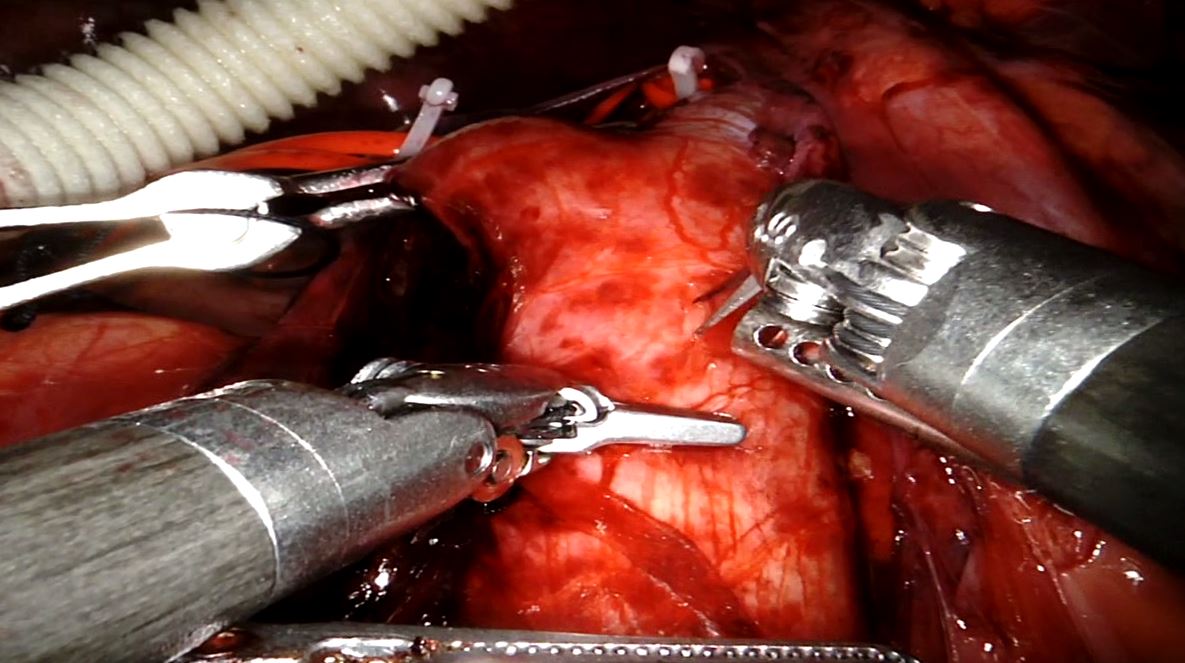
RESULTS: After induction of general anesthesia, she was placed a supine position. Standard sterile prep and drape was performed. Four robotic ports were inserted in the lower abdomen (Two 8 mm, one 12 mm, and one 5 mm). The robotic surgical system was docked and connected to the ports. The peritoneum overlying the right internal and external iliac arteries was incised. Cephalad dissection was carried out to ensure adequate proximal vascular control. The right ureter was retracted laterally. A 10mm Dacron graft was inserted through the 12mm port. A laparoscopic Debakey clamp was placed on the proximal common iliac artery. An end to side anastomosis to the common iliac artery was performed with a 2-0 Gore-Tex suture in running fashion. Next, a right groin incision was made and the common femoral, superficial femoral and profunda femoris arteries were dissected. A retroperitoneal tunnel was made bluntly from the femoral exposure site into the abdomen in an anatomic plane. The distal end of the graft was retrieved into the femoral wound under direct vision from inside the abdomen. An end to side anastomosis to the common femoral artery was performed with a 5-0 prolene suture. Once flow was restored, excellent inflow and pulse was appreciated in the distal arteries. The groin and port sites were closed in standard fashion. The estimated blood loss was 70ml. The total operative time was 233 minutes. She was discharged on postoperative day 1.
CONCLUSIONS: Robotic assisted ilio-femoral bypass grafting is a safe and feasible minimally invasive alternative to an open retroperitoneal dissection for the treatment of iliac artery endofibrosis. This is particularly important for patients who desire a shorter recovery for lifestyle or work related reasons. 
Back to 2018 Abstracts



