
Association Of Preoperative Spinal Drainage Placement With Spinal Cord Ischemia Among Patients Undergoing Thoracic Endovascular Aortic Repair
Alejandro Suarez-Pierre, Xun Zhou, Jose E Gonzalez, Muhammad Rizwan, Charles D Fraser, III, Cecillia Lui, Mahmoud B Malas, Christopher J Abularrage, James H Black, III
Johns Hopkins University, Baltimore, MD
BACKGROUND: Spinal cord ischemia (SCI) is among the most devastating complications of thoracic endovascular aortic repair (TEVAR). Spinal fluid drainage has been proposed as a viable means to reduce SCI, but few data exist to support its routine use. This study investigated the association of preoperative spinal fluid drainage with risk of SCI after TEVAR.
METHODS: The Vascular Quality Initiative TEVAR module was queried for adult patients (≥18 years), undergoing TEVAR (coverage of zones 0-5), between September 2014 and March 2018 (inclusive). Patients with preoperative spinal malperfusion, aortic rupture on presentation, and connective tissue disorders were excluded. One-to-one propensity-matching was used to balance patients on 44 separate dimensions, via the nearest-neighbor principle to compare those with versus without preoperative spinal drainage. The primary endpoint was spinal cord ischemia still present at the time of discharge. Secondary outcomes were 30-day mortality and prolonged ICU stay (>7 days).
RESULTS: Among 4,287 patients who underwent TEVAR (mean age 67.1 [SD 13.7] years, 1,665 [38.8%] women, and 2,622 [61.2%] men), 2,076 had a spinal drainage placed. Propensity-matching yielded 1,292 pairs with adequate covariate balance (all 44 absolute standardized differences <0.1). In the 2,584 propensity-matched patients, spinal drainage placement was associated with a reduced risk of SCI (1.5% vs 2.5%, risk-adjusted odds ratio [OR] 0.47 [95% CI 0.24-0.89], p=0.02). The rates of 30-day mortality (4.5% vs 5.0%, risk-adjusted OR 0.67 [95% CI 0.44-1.01], p=0.05) and prolonged ICU stay (7.0% vs 5.7%, risk-adjusted OR 1.10 [95% CI 0.84-1.45], p=0.48) did not differ based on spinal drainage placement.
CONCLUSIONS: Among patients undergoing thoracic endovascular aortic repair, preoperative placement of a spinal drainage, compared with no drainage, was associated with reduced risk of spinal cord ischemia. Further investigation, including randomized controlled trials, is needed to more definitively determine the role for spinal drainage in TEVAR. 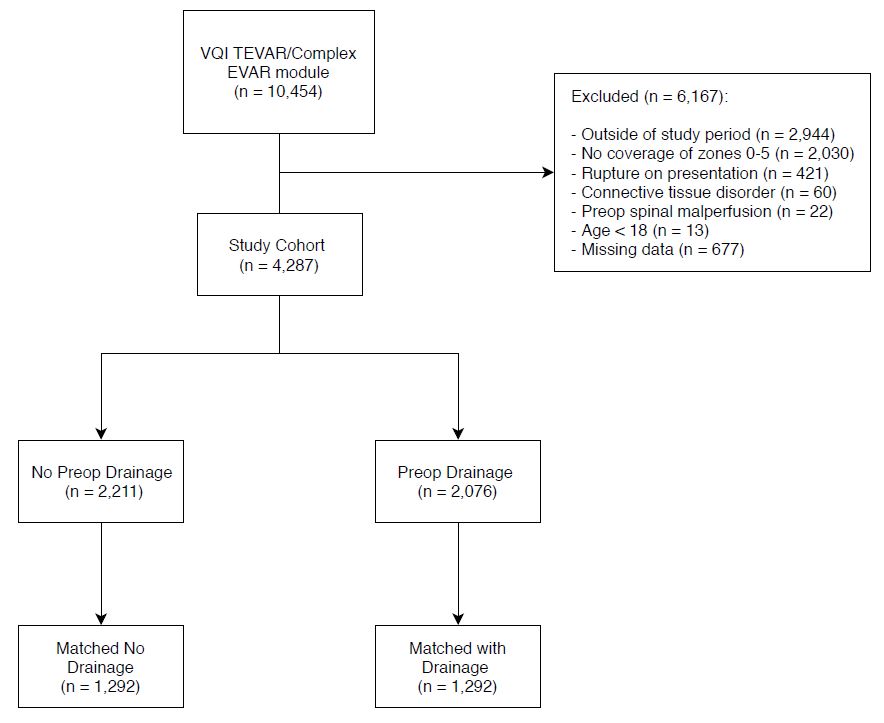
Back to 2019 Abstracts