
Posterior Tibial Vein Aneurysm Masquerading as a Baker’s Cyst
Hunter M Ray, Juan B Umana Pizano, Paul G Haddad, Stuart A Harlin
The University of Texas Health Science Center at Houston (UT Health), McGovern Medical School, Houston, TX
INTRODUCTION:
Venous aneurysms have a poorly defined natural history and are often only discovered when they lead to local symptoms or pulmonary embolic complications.
METHODS:
Here we present the case of an otherwise healthy gentleman with right lower extremity pain of acute onset without known provocative event who was determined to have a symptomatic posterior tibial vein aneurysm.
RESULTS:
A 45-year-old otherwise healthy man presented to the vascular surgery clinic for further workup of his acute onset right lower extremity pain and swelling which had begun abruptly 3 months prior to presentation without recent or remote history of trauma or extremity injury. In the time preceding evaluation by vascular surgery the patient had visited the emergency department and undergone an ultrasound with the report noting a hypoechoic cystic structure present in the posteromedial knee/ proximal calf measuring 2.8x1.6x1.9cm reported to be consistent with Baker’s cyst. The ultrasound report noted that there was no irregularity of deep or superficial veins of the lower extremity. The patient was referred to orthopedic surgery for further evaluation and underwent magnetic resonance imaging (MRI) of the knee with evidence of mild degenerative disease, but without evidence of a Bakers cyst. The MRI did show a small area concerning for vascular malformation which lead the patient to present to our vascular surgery clinic. On examination the patient had a painful palpable mass along the right medial posterior leg worsened with prolonged standing, and right lower extremity CEAP C4a disease. A venous duplex ultrasound (US) obtained in our ICAVL lab. US images revealed a 1.8x3.9x1.7cm posterior tibial vein aneurysm (Images 1 and 2) with sluggish flow noted. The study also demonstrated presence of significant bilateral greater saphenous vein (GSV) and right lesser saphenous vein (LSV) reflux. Comparison of the two ultrasounds demonstrates the misdiagnosis with the initially diagnosed "Baker’s cyst" truly being a posterior tibial vein aneurysm. The patient is currently doing well and scheduled for ablation of refluxing superficial veins, symptomatic treatment with rest and compression and a plan to reimage after venous ablation to reassess the aneurysm.
CONCLUSIONS:
Venous aneurysms are rare, however with proper physical exam and appropriate imaging they can be easily diagnosed. This study highlights the importance of quality ultrasound and experienced technicians in the diagnosis of a rare disease. Management of venous aneurysms is determined on a case-by-case basis and depends on the location and severity of symptoms. Further study is needed to better characterize the natural history of venous aneurysmal disease.
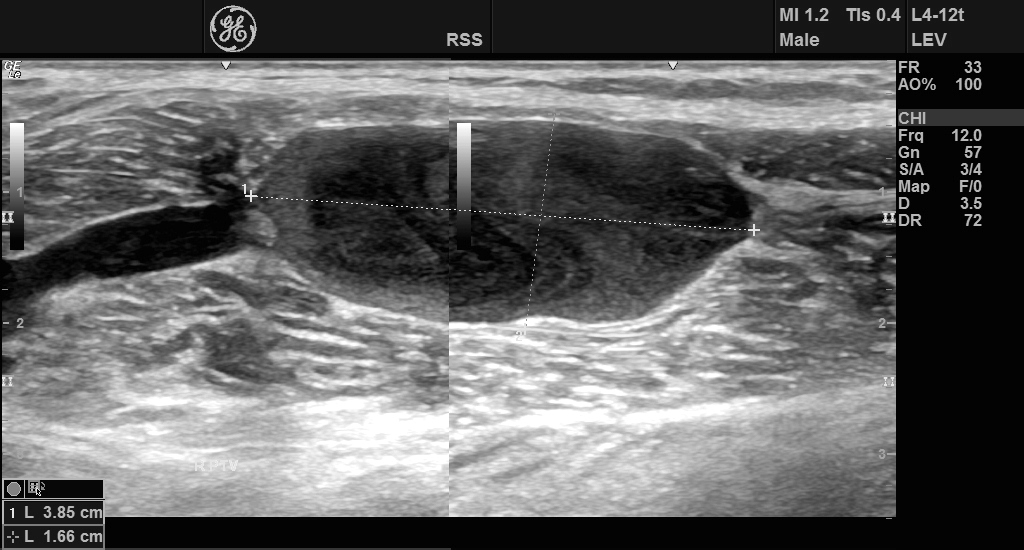
Image 1: B-mode ultrasound image demonstrating right posterior tibial vein aneurysm
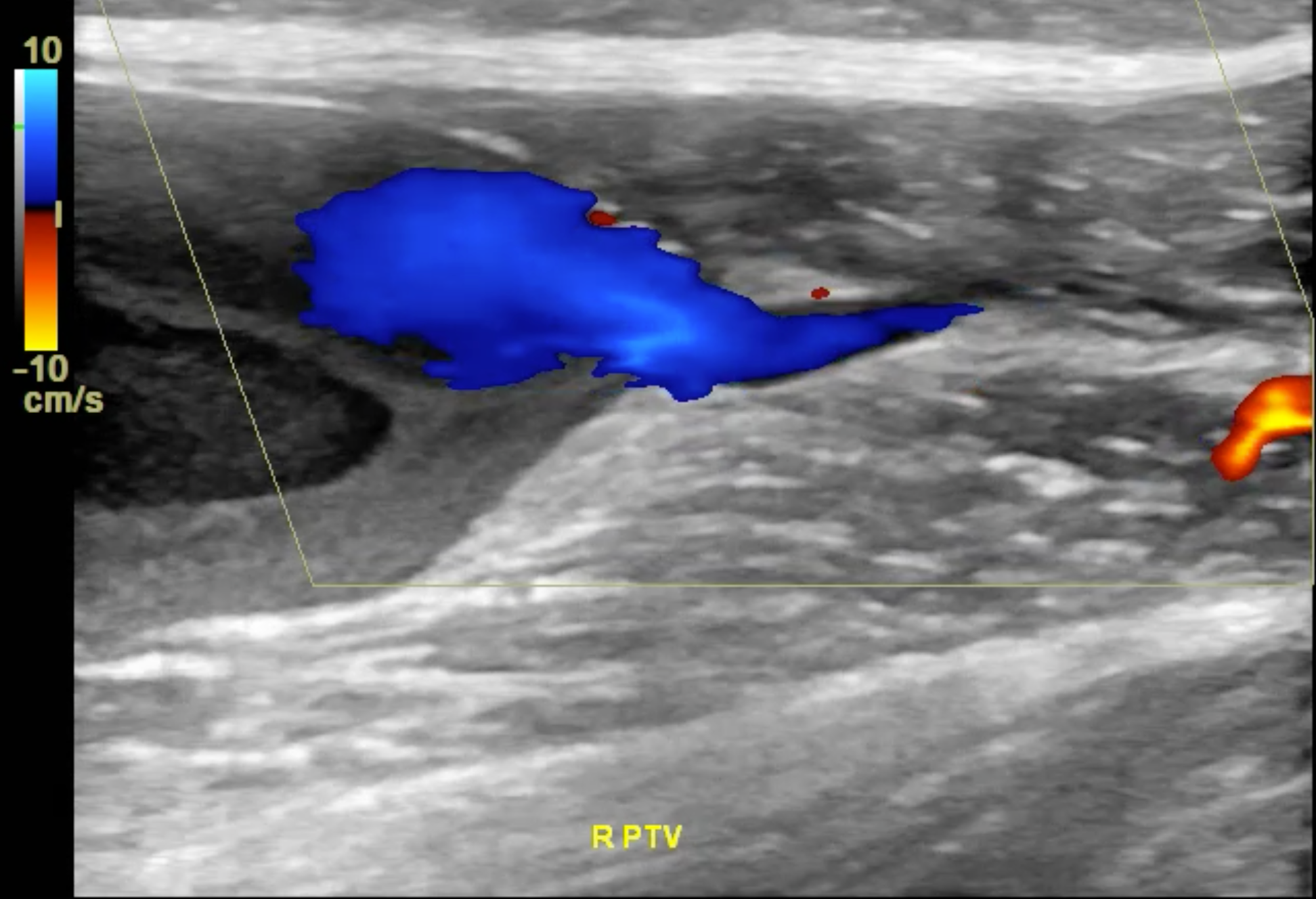
Image 2: Colorflow ultrasound image of right posterior tibial vein aneurysm with augmentation
Back to 2019 Abstracts