
Modifications of the "Inside-Out" Technique for Re-establishing Left Subclavian Venous Access
Charles S Kiell, Robert A McCready
Franciscan Indianapolis, Indianapolis, IN
Background: Central venous occlusion poses a challenge to the placement of new devices such as dialysis catheters or pacemaker leads. Previous descriptions of the "inside-out" technique for venocutaneous access have focused on directing the stiff end of a 0.14 wire toward the right supraclavicular fossa, highlighting the relatively straight trajectory it affords. Achieving access through an occluded left subclavian vein poses different challenges because the vein takes a horizontal and somewhat posteriorly oriented course. Retrieving the wire using the "inside-out" technique may be difficult due to the wire’s tendency to follow the course of the vein. Re-establishing this route is particularly desirable for pacemaker lead placement as supraclavicular or transthoracic tunneling pose increased risk of lead dislodgement or fracture.The TourGuide sheath (Medtronic, Minneapolis, MN) is a 90cm long steerable 6.5Fr sheath that allows controlled tip deflection by rotating a dial on the handle. Deflection angles of up to 180 degrees with firm support can be achieved. The tip of the sheath also has a circular radiopaque marker. Using tip deflection and rotation of the image intensifier, a coaxial, "down the barrel" view of the sheath tip can be easily achieved. This view allows predictable guidewire trajectory. Methods: Femoral access is achieved with ultrasound guidance. Using standard guidewire and catheter exchanges, a 90cm long TourGuide sheath is placed at the point of obstruction in the subclavian vein. A hemostat is placed on the skin at the desired exit point. The gantry angle of the image intensifier is then manipulated so that the tip of the hemostat and radiopaque marker of the sheath are coaxially aligned. The TourGuide sheath tip is then rotated anteriorly so that the circular tip marker is fully developed and a "down the barrel" view is obtained. Once this configuration is achieved, the back end of an 0.14 300cm guidewire is used to traverse the venous occlusion, soft tissues and then become identifiable by tenting of the skin. The guidewire is retrieved through a small incision is made over this point and then working access is achieved using conventional guidewire and sheath exchanges. Alternatively, the wire can be retrieved by open exposure if open pacemaker revision is required. Results:We have successfully accomplished pacemaker lead revision is 3 patients with axillo-subclavian occlusion without complications. Conclusions:The ‘inside-out" technique is a useful method for re-establishing central venous access. Our preliminary results suggest that the technical modifications described herein can allow for safe and successful device revisions using the occluded left axillosubclavian vein and could be utilized for placement of dialysis access or other central venous catheters. The TourGuide sheath adds stability and steerability for reliable guidewire penetration and trajectory. Addition of these modification to the "inside-out" arsenal extends the anatomical domain and adds safety to current methods. 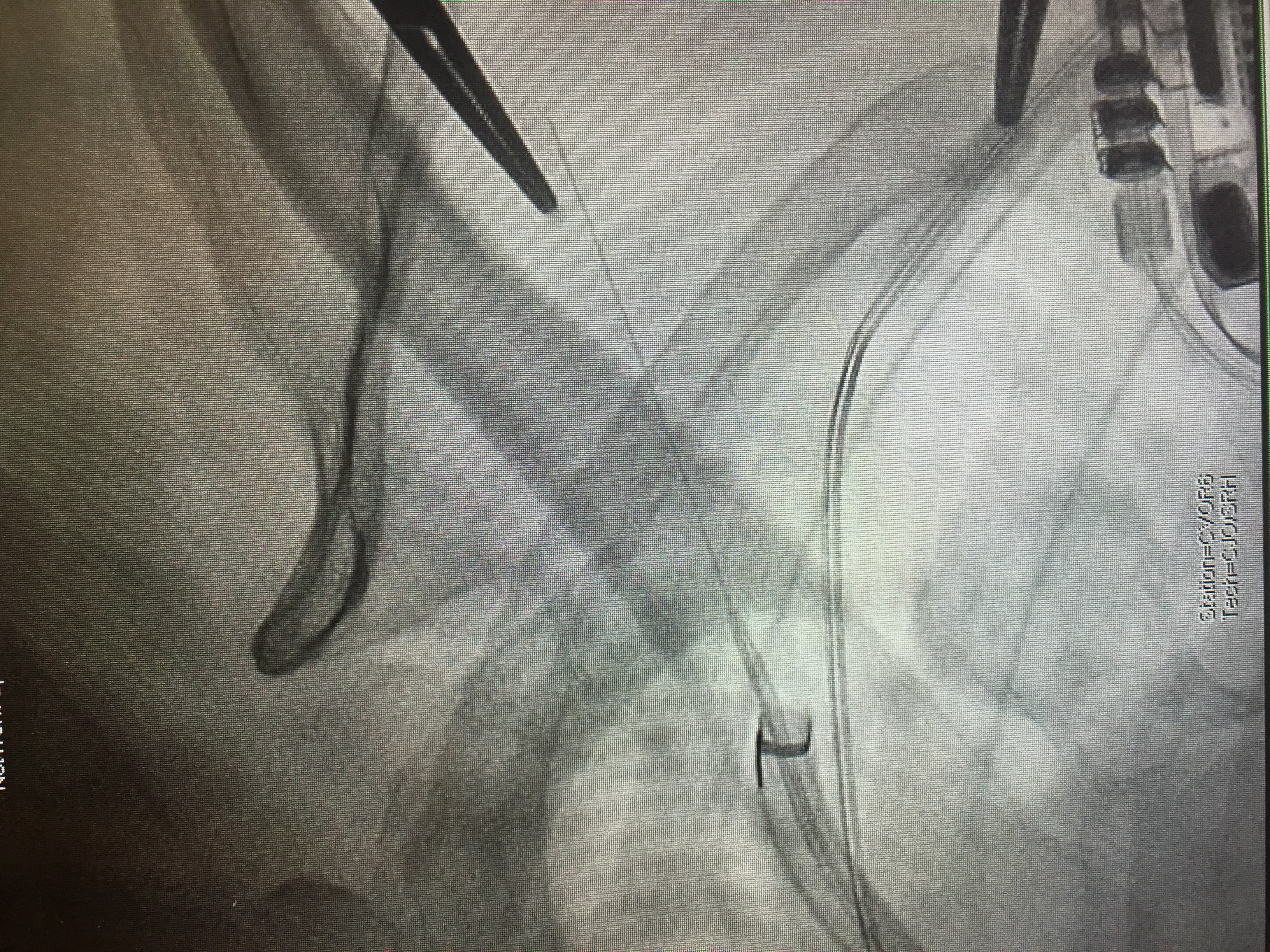
Back to 2019 Abstracts