
Artery of Adamkiewicz Preservation During Fenestrated-Branched Endovascular Aortic Aneurysm Repair (F-BEVAR)
Anna L. Driessen, Carla K. Scott, Gerardo G. Guardiola, Mirza S. Baig, Melissa L. Kirkwood, Carlos H. Timaran
UT Southwestern Medical Center, Dallas, TX
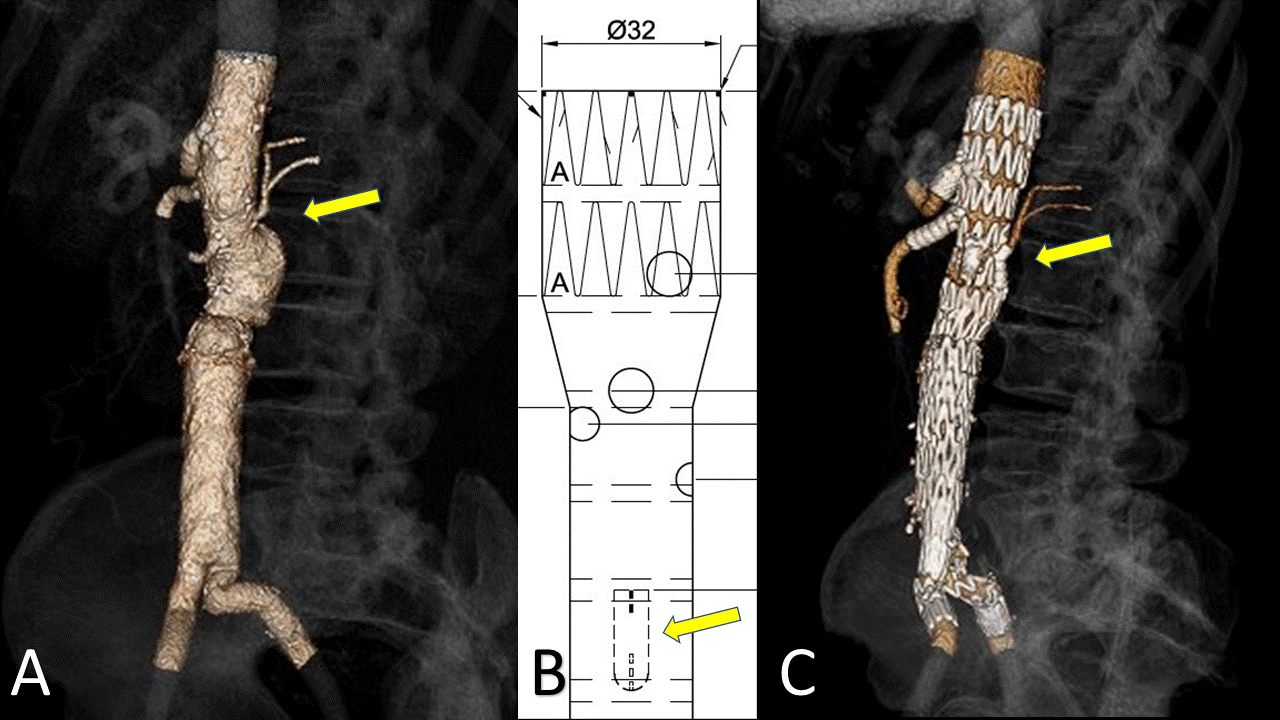
BACKGROUND: The exclusion of lumbar and intercostal arteries, specially the artery of Adamkiewicz, plays an important role in the development of spinal cord ischemia during complex endovascular aortic aneurysm repair. We present a case of a patient with a complex abdominal aortic aneurysm who underwent F-BEVAR using a patient specific device with an additional branch for preservation of the artery of Adamkiewicz. METHODS: A 75-year-old male patient developed a suprarenal abdominal aortic aneurysm (AAA) after prior open aortobifemoral repair for an infrarenal AAA. The computed tomography angiogram (CTA) demonstrated proximal aneurysmal degeneration with a 6.2cm suprarenal AAA. A large artery of Adamkiewicz was evident just above the origin of the renal arteries (Fig A) as well as bilateral occlusion of the internal iliac arteries. Because of the comorbidities and prior open repair, an endovascular repair was recommended. Accordingly, an investigational patient specific device was designed with 4 fenestrations for the visceral and renal vessels and an additional 6 x18 mm upward facing branch for the artery of Adamkiewicz (Fig B). Bilateral percutaneous and right open brachial access was obtained. The fenestrated-branched device was deployed sequentially while selecting the visceral arteries. The upward branch was selected using a steerable sheath from the right femoral access. The Adamkiewicz artery was then catheterized and stented with a covered balloon expandable stent (Gore VBX 5x39mm). The procedure was successfully completed with the deployment of the bifurcated graft and iliac extensions. Completion angiogram showed excellent technical result with perfusion of all visceral arteries and the artery of Adamkiewicz with no significant endoleak. Intraoperative neuromonitoring demonstrated no changes in sensory and motor evoked potentials. Near-infrared spectroscopy revealed stable and unchanged oxygen saturation at all levels perioperatively.
RESULTS: The post-operative course was unremarkable and without any neurological alterations. The 30-day follow-up CTA demonstrated patent fenestrated endograft and stents without evidence of endoleak. The artery of Adamkiewicz and its branch were patent with good flow into both branches of the artery (Fig C). CONCLUSION: We here describe the first case reported in the literature using a patient specific device designed with an upward facing branch to preserve the flow into the artery of Adamkiewicz. This technique should be considered to decrease the risk of spinal cord injury during complex endovascular aneurysm repair when the anatomy for preservation is feasible and the spinal cord collateral arterial network is incomplete.
Back to 2021 Abstracts