
Contemporary Outcomes of Aortobifemoral Bypass with Concomitant Lower Extremity Bypass in the Vascular Quality Initiative
Luke M. Stewart, Graeme E. McFarland, Emily L. Spangler, Marc A. Passman, Benjamin J. Pearce, Mark A. Patterson, Danielle C. Sutzko, William F. Gaillard, Zdenek Novak, Adam W. Beck
University of Alabama at Birmingham, Birmingham, AL
INTRODUCTION: Aorto-bi-femoral bypass (ABF) is the gold standard for open surgical management of aortoiliac occlusive disease. Although as many as half of patients have additional significant infrainguinal atherosclerotic disease, few are treated with concomitant lower extremity bypass (LEB) unless there extenuating circumstances. There is limited contemporary data regarding outcomes of ABF + LEB consisting of small, single institution series comparing outcomes between ABF alone and ABF+LEB. We aim to compare the rate of mortality, major perioperative complication, freedom from occlusion, and freedom from major amputation between ABF alone and ABF+LEB in a large national registry.METHODS: The Vascular Quality Initiative (VQI) suprainguinal bypass module was used to identify patients undergoing elective ABF for occlusive disease from 2009-2019. Patients undergoing ABF for aneurysm, acute limb ischemia, or urgent/emergent procedures were excluded. The primary outcomes were rates of major perioperative complication and 30-day mortality. Multivariable regression was performed including all variables with p<.10 on univariate analysis to evaluate for demographic and perioperative predictors of 30-day mortality and perioperative major complication. Kaplan Meier analysis was used to estimate postoperative survival.RESULTS: 5,495 ABF patients were identified with 209 undergoing concomitant LEB (3.8%). Major complications occurred in 22.5% of the ABF+LEB cohort compared to 15.2% in isolated ABF (p<.01). 30-day mortality was increased in the ABF+LEB cohort (ABF+LEB: 7.2%, ABF: 2.0%; p<.01). On multivariable analysis, ABF+LEB remained associated with major complications (OR: 1.42, 95% CI: 1.01-2.01; p=.05) as well as higher 30-day mortality (OR: 2.74, 95% CI: 1.26-5.98; p=.01). Other factors associated with 30-day mortality on multivariable analysis included female gender, extubation after leaving the operating room, postop vasopressor
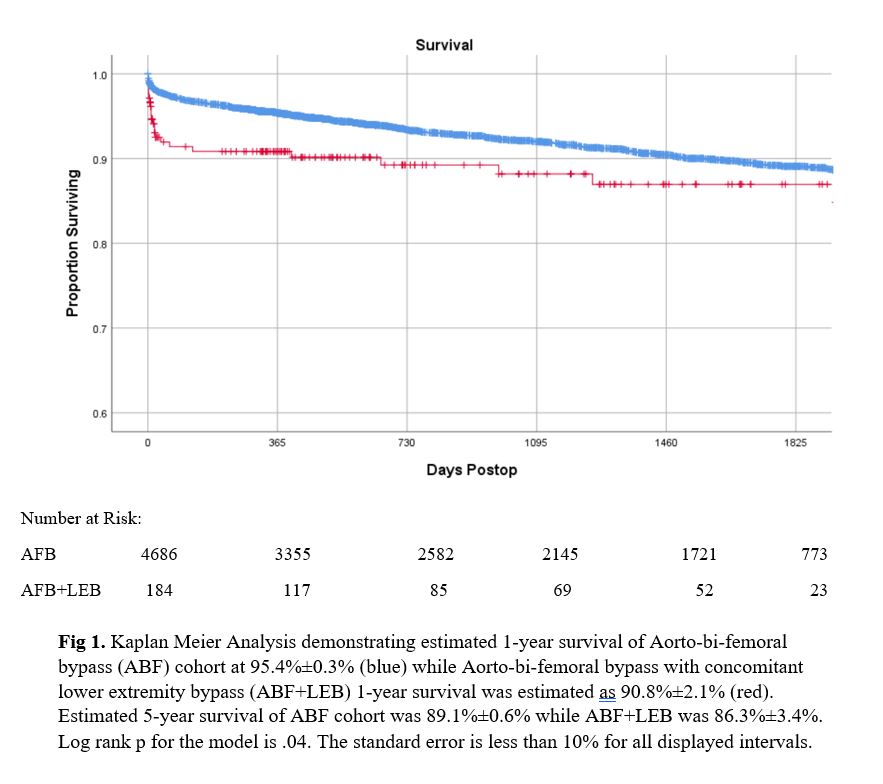
requirement, renal complication, MI, and respiratory complication. Other variables associated with the occurrence of a perioperative major complication included preoperative CHF, HTN, ASA Class ≥4, prior inflow bypass, concomitant femoral endarterectomy, or not being independently ambulatory preop. Kaplan Meier estimated survival was decreased in the ABF+LEB cohort at 1-year (ABF+LEB: 90.8% ± 2.2%, ABF: 95.4% ± 0.3%; p=.04) (Fig 1). Primary patency of the ABF graft at discharge from the index hospitalization was also decreased in the ABF+LEB cohort (ABF+LEB: 92.5%, ABF: 96.4%; p=.01). CONCLUSION: Aorto-bi-femoral bypass with concomitant lower extremity bypass is associated with increased rates of perioperative major complications and 30-day mortality when compared to ABF alone, but has acceptable long-term survival and patency. Although the decision to perform ABF + LEB is highly patient and presentation dependent, when combined, these procedures have a significant physiologic impact and mortality, and ABF + LEB should be performed only in select patients.
Back to 2021 Abstracts