
Back to 2016 Annual Meeting Program
Flexible robotics with electromagnetic tracking improve safety and efficiency during in vitro endovascular navigation
Adeline Schwein1, Ben Kramer2, Ponraj Chinna Durai3, Sean Walker4, Marcia O'Malley2, Alan Lumsden1, Jean Bismuth1
1Houston Methodist Hospital, Houston, TX;2Rice University, Houston, TX;3Siemens Medical Solution USA Inc, Hoffman Estates, IL;4Hansen Medical Inc, Montain View, CA
INTRODUCTION:One limitation of the remotely steerable robotic catheter (Magellan™, Hansen Medical Inc., Mountain view, CA) is the lack of real-time 3D localization: it is still being navigated based on 2D X-ray fluoroscopic projection images. Our goal was to evaluate if incorporating an electromagnetic (EM) sensor in the robotic catheter tip can overcome this limitation and potentially improve endovascular navigation.
METHODS:Six users with varied experience in robotic endovascular procedures, were tasked to navigate using the 9Fr robotic catheter, with EM sensors incorporated at the tip of leader, in a fluid-filled aortic aneurysm phantom. An EM field was generated by a device under the angiography table. All users cannulated two anatomical targets (left renal artery and a “gate” located towards the posterior aspect of the model) using 4 different visualization modes (Figure 1):
(1) Standard fluoroscopy mode (Control)
(2) 2D biplane fluoroscopy mode showing real-time virtual catheter orientation from EM tracking
(3) 3D VRT model (AP-view) of phantom and endo-luminal view showing virtual catheter orientation from EM tracking
(4) 3D VRT model (AP and lateral view) showing virtual catheter orientation from EM tracking
Standard X-ray fluoroscopic imaging was always available. Cannulation and fluoroscopy times were noted for every mode. 3D positions of the tip sensor were recorded at 4 Hz to establish and measure catheter trajectories. Kinematic metrics including number of submovements, spectral arc length and dimensionless jerk, were calculated to assess the consistency of the catheter motion. A contrast t-test was used to compare standard fluoroscopy mode to the use of EM tracking.
RESULTS:The EM sensor incorporated catheter navigated as expected according to all users. The success rate for cannulation was 100%. For the posterior gate target, mean cannulation times (mm:ss) were 8:12, 4:19, 4:29 and 3:09 respectively for the modes 1, 2, 3 and 4 (p=0.013). Mean fluoroscopy times were 274, 20, 29 and 2 seconds respectively (p=0.001). Mean 3D path lengths were 1046, 446, 441 and 417 mm respectively (p=0.009). Spectral arc length, dimensionless jerk and number of submovements were all significantly reduced when using EM tracking for the posterior gate cannulation (p<0.05) (Table 1), showing higher quality of movement.
CONCLUSIONS:Electromagnetically tracked Magellan robotic catheter allowed better real-time 3D orientation, facilitating navigation, with reduction in cannulation and fluoroscopy times and improvement in motion consistency. Although this is preliminary work, it has the potential to improve procedural safety and efficacy, and to lead towards “fluoroscopy free” endovascular surgery. 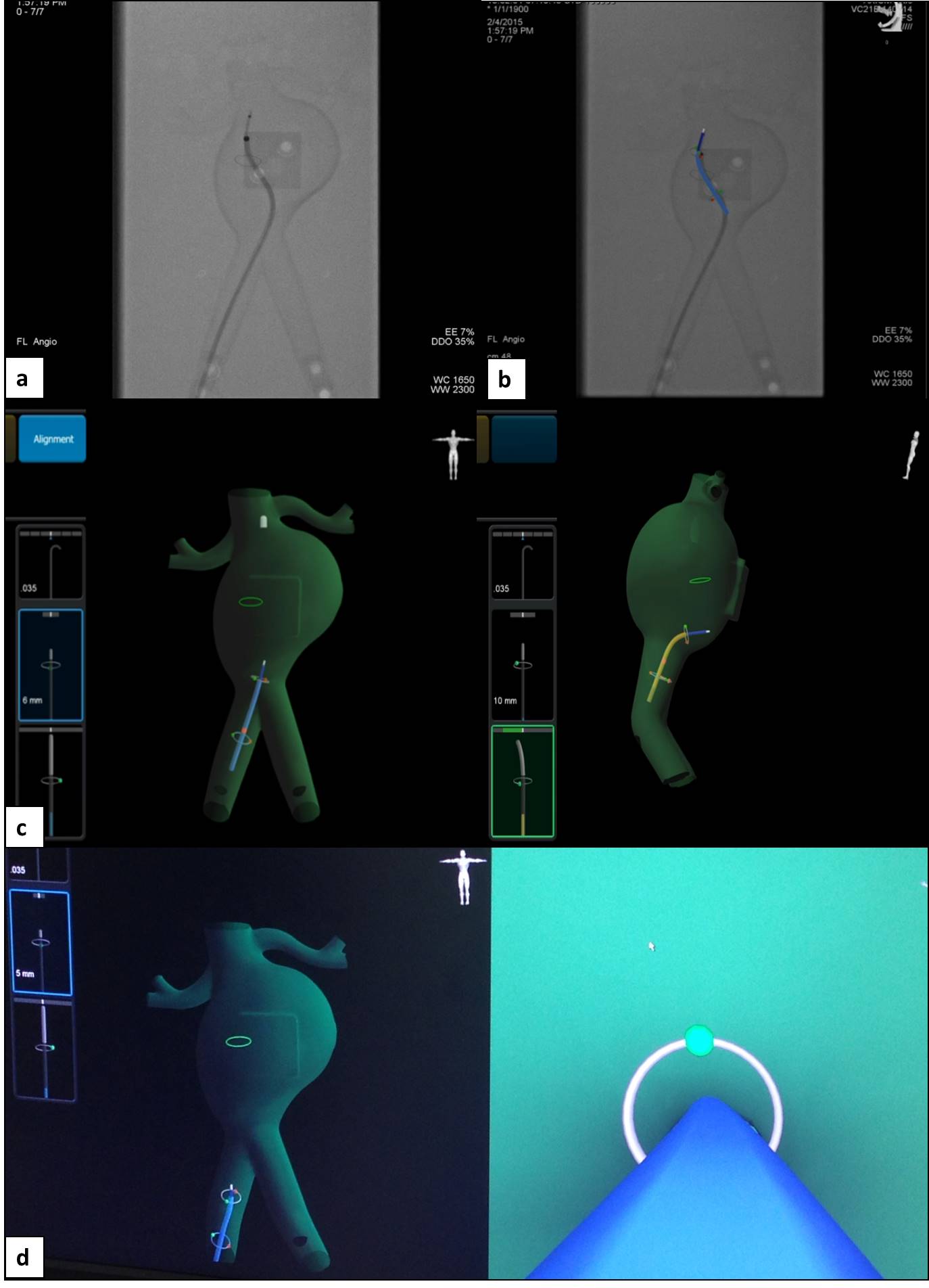
| mode 1 | mode 2 | mode 3 | mode 4 | p | |
| Fluoroscopy time (seconds) | 274 | 20 | 29 | 2 | 0.001 |
| Cannulation time (min:sec) | 08:12 | 04:19 | 04:29 | 03:09 | 0.013 |
| 3D pathway (mm) | 1043.4 | 445.8 | 441.0 | 417.2 | 0.009 |
| Spectral Arc Length | -13.8 | -10.9 | -9.5 | -9.1 | 0.017 |
| Dimensionless Jerk | 612924.0 | 315650.2 | 219863.1 | 217938.8 | 0.009 |
| Number of Submovements | 37.2 | 19.7 | 19.5 | 15.5 | 0.002 |
Back to 2016 Annual Meeting Program