
Differences In Procedural Metrics And Clinical Outcomes Among Patients Treated By Fenestrated-Branched Endovascular Repair Of Thoracoabdominal Aortic Aneurysms Using Infrarenal Aortic Versus Iliac Sealing Zones
Guilherme B. Lima1, Emanuel R. Tenorio1, Giulianna B. Marcondes1, Thanila A. Macedo1, Naveed Saqib1, Sophia Khan1, Bernardo C. Mendes2, Gustavo S. Oderich1
1University of Texas Health Science Center at Houston, McGoven Medical School, Houston, TX, Houston, TX, 2Mayo Clinic, Rochester, MN
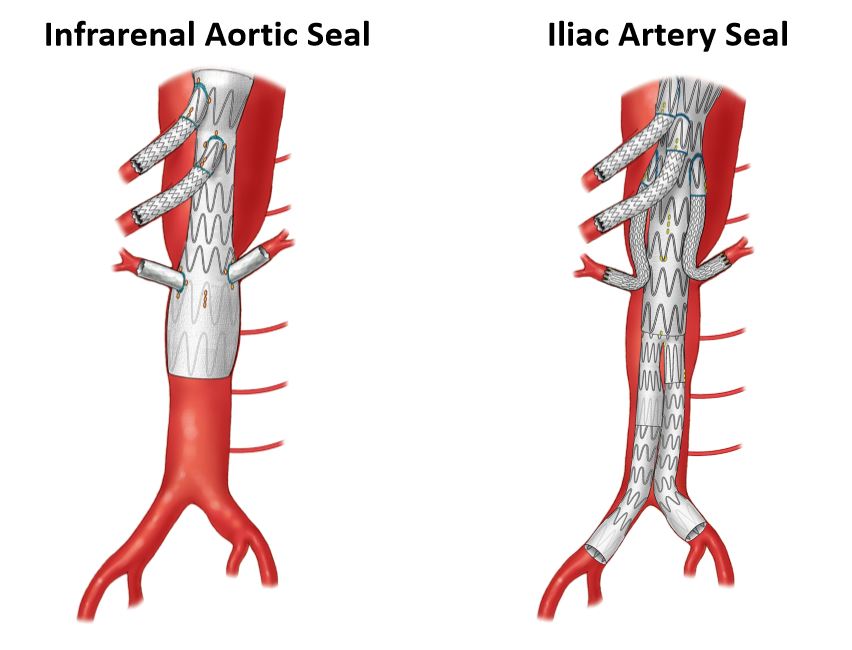
Purpose: Use of infra-renal aortic versus iliac sealing zone (Figure) during fenestrated-branched endovascular aortic repair (FB-EVAR) allows salvage of lumbosacral arteries and early lower extremity reperfusion, but may add risk of Type Ib endoleak (TIbE). The purpose of this study was to assess outcomes of FB-EVAR using infrarenal aortic versus iliac sealing zones. Methods: We reviewed the clinical data of 430 consecutive patients enrolled in a prospective non-randomized study to evaluate FB-EVAR between 2013-2020. Patients with prior infrarenal open or endovascular grafts and pararenal aneurysms were excluded. Outcomes were analyzed in patients with Extent I-IV TAAAs who underwent FB-EVAR with distal device implantation in the infrarenal aorta or iliac arteries. End-points were 30-day or in-hospital mortality, major adverse events (MAEs) and freedom from TIbE, freedom from secondary interventions and changes in infra-renal aortic neck diameter. Results: There were 94 patients (46 males, mean age 73±8 years-old) included in the study. Distal sealing zone was obtained in the infrarenal aorta in 53 patients (56%) or iliac arteries in 41 patients (44%). Both groups had similar clinical characteristics, aneurysm extent and diameter, except for more female patients treated with infrarenal aortic sealing zone (60% vs 39%, p= .04) and higher serum creatinine among those who had iliac sealing zone (1.24±0.6 vs 1.01±0.3, p=.02). Technical success was obtained in 90 patients (96%) with no difference between groups. Use of infrarenal aortic sealing zone was associated with shorter operating time (243±80 vs 271±68 min, p=.08), shorter fluoroscopy time (77±28 vs 94±35 min, p=.008), lower cumulative air kerma (1409±1423 vs 2284±1409 mGy, p=.005) and lower dose area product (154±77 vs 211±99 Gy.cm2, p=.03). There were no 30-day or in-hospital mortality. There was no difference in MAEs among patients treated with infrarenal aortic vs iliac sealing zones (24% vs 37%, P 0.20), including SCI (9% vs 7%, p=.67), respectively. Mean follow up was 29±20 months. TIbE occurred in one patient in each group (2% vs 2%, p=1.0). Freedom from TIbE and freedom from secondary intervention was 98±2% and 67±8% for patients who had infrarenal aortic sealing zone and 97±3% and 69±9% for those who had iliac sealing zone at 3-years, respectively (P=NS). The mean infrarenal aortic diameter enlargement at the distal sealing zone was 5±3.2 mm at 3 years. There were no late TIbE due to progression of disease in the infrarenal aorta. Conclusion: Use of infrarenal aortic or iliac artery seal zone is equally safe and effective during FB-EVAR, provided patients have suitable segments. The use of infrarenal aortic sealing zone has modest procedural advantages such as shorter operating and fluoroscopy time and lower effective radiation dose. There was no difference in clinical outcomes and TIbEs.
Back to 2021 Abstracts