
IgG4-Related Symptomatic Abdominal Aortic Aneurysm in a Patient with Known Myasthenia Gravis
Lauren Haney, Allison Laffoon, Lalithapriya Jayakumar, Dimitrios Miserlis, Fermin Tio, Lisa Radkay-Gonzalez, Lori Pounds, Reshma Brahmbhatt
UT Health San Antonio, San Antonio, TX
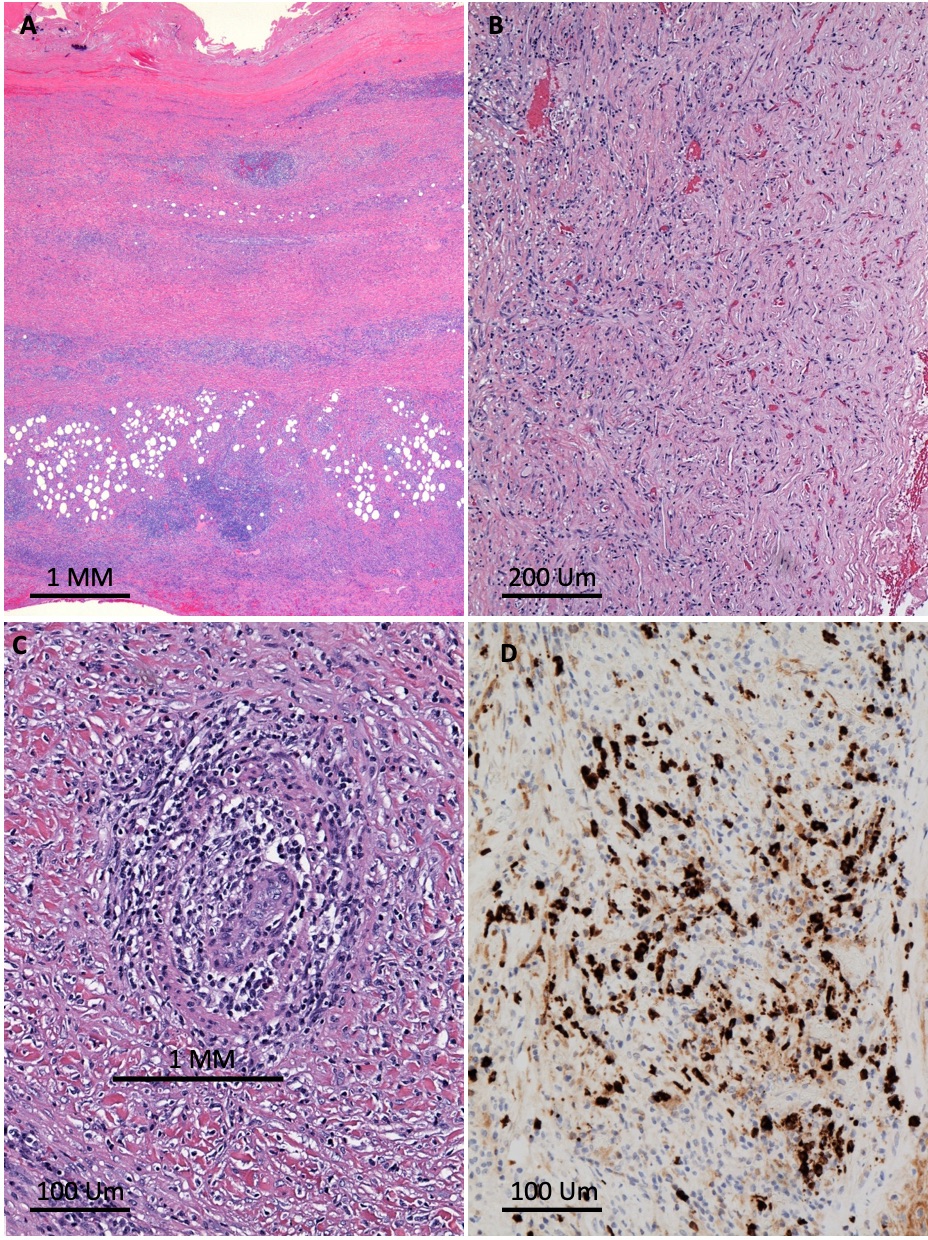
Background: IgG4-related disease is an inflammatory cause of fibrosis and sclerosis of several organs, including the aorta and other medium-to-large arteries. An association has been found between IgG4-related disease and autoimmune disease. We present a patient with a history of myasthenia gravis and acute presentation of a symptomatic IgG4-related inflammatory aneurysm (IAAA).Methods: A 59-year-old man presented to the ED with severe abdominal pain radiating to his back. Imaging was consistent with an 8cm juxtarenal AAA with findings concerning for infection and impending rupture. He was taken to the operating room emergently for open repair with a Rifampin-soaked Dacron aortoiliac reconstruction.Results: Pathology of the aneurysm wall was consistent with IgG4-related disease. He was referred to rheumatology and started on anti-inflammatory therapy with Prednisone and Azathioprine. One-year postoperative imaging revealed no residual inflammatory changes and a patent reconstruction.Conclusions: IgG4-related disease has been increasingly described as a cause of inflammatory AAA over the last decade. Similar imaging and macroscopic findings between IgG4-related and infectious AAA have led to open repair in reported cases followed by histologic diagnosis. Ongoing research is directed at finding a non-invasive marker of disease to allow for early treatment with anti-inflammatory therapies to reduce rupture risk and help guide the type of surgical intervention offered to these patients.

Back to 2021 Abstracts