
Back to 2017 Annual Meeting Program
Outcomes of Thoracic Endovascular Aortic Repair in Adult Aortic Coarctation Patients
Satish H. Chandrasekhar1, Salvatore T. Scali1, Salim Lala1, Kristina A. Giles1, Adam W. Beck2, Javairiah Fatima1, Scott A. Berceli1, Thomas S. Huber1, Robert J. Feezor1
1University of Florida- Gainesville, Gainesville, FL;2University of Alabama-Birmingham, Birmingham, AL
INTRODUCTION: Although aortic coarctation is most commonly seen in pediatric patients, adults can present with late sequelae of untreated coarctation or complications of the index repair. To date, there are limited data about the role of thoracic endovascular aortic repair (TEVAR) in this group of patients. The purpose of this analysis is to describe our experience with management of adult coarctation patients treated with TEVAR.
METHODS: A retrospective review was completed of a prospectively maintained endovascular aortic registry at a university hospital. All patients treated for primary coarctation or for late sequelae of previous open repair (e.g. pseudoaneurysm, recurrent coarctation/anastomotic stenosis related to index open coarctation repair) were included. Patient demographics, comorbidities, procedure related variables, postoperative outcomes, and reintervention were abstracted. Computed tomographic centerline assessments of endograft morphology were also completed to delineate stent anatomy at the site of coarctation. Survival was estimated using Kaplan-Meier life tables.
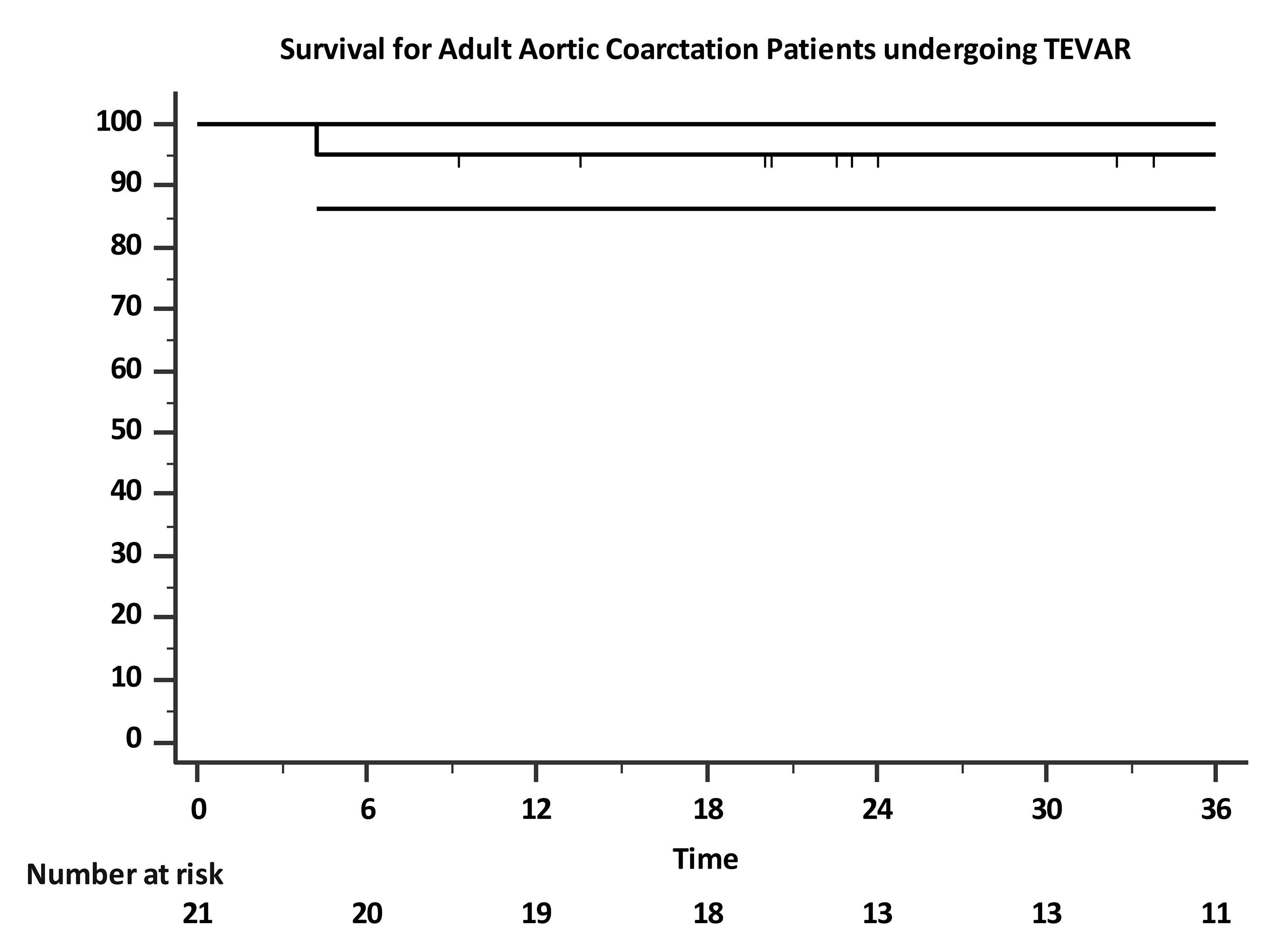
RESULTS: A total of 21 patients were identified [median age = 46 years (range 33-71); 67% male (n=14)]. Nine patients (43%) were treated for symptomatic primary (n=6) or recurrent coarctation (n=3). Other indications included: degenerative thoracic aneurysm (n=6), pseudoaneurysm (n=4), and dissection (n=2). Zone 1 or 2 landings were employed in 15 patients (zone 2, n=13; zone 1, n=2). Additional procedure related data is depicted in the Table. No 30-day mortality events occurred and 2 patients (10%) experienced a postoperative complication (non-disabling stroke, n=2). At a median clinical follow-up time of 8 months [range 1-106], 3 endoleaks were detected, all of which were type 2 related to patent left subclavian (n=2) or aberrant subclavian arteries (n=1). Four patients (19%) underwent reintervention (median time: 7 months [range 2-12]) and 3 out of 4 of these were subclavian artery embolizations, while one was for aortic root replacement due to pre-existing bicuspid aortic valve with concomitant ascending aortic aneurysm. In patients with available CT imaging (n = 6 of 9 primary/recurrent coarctation subjects), nominal stent diameters at the site of coarctation were effectively achieved within these patients (range -0.4 to -1.2mm of desired final stent diameter). One and 3-year survival is estimated to be 95±5% (Figure). One late death occurred related to complications from pre-existing congenital heart disease.
CONCLUSIONS: Adult patients with aortic coarctation can be treated safely with TEVAR. The annular constriction of an aortic coarctation can be successfully dilated by the self-expanding stent graft. Greater patient numbers and longer term follow-up are needed to further define the role of TEVAR in the management adult patients with complications of aortic coarctation. 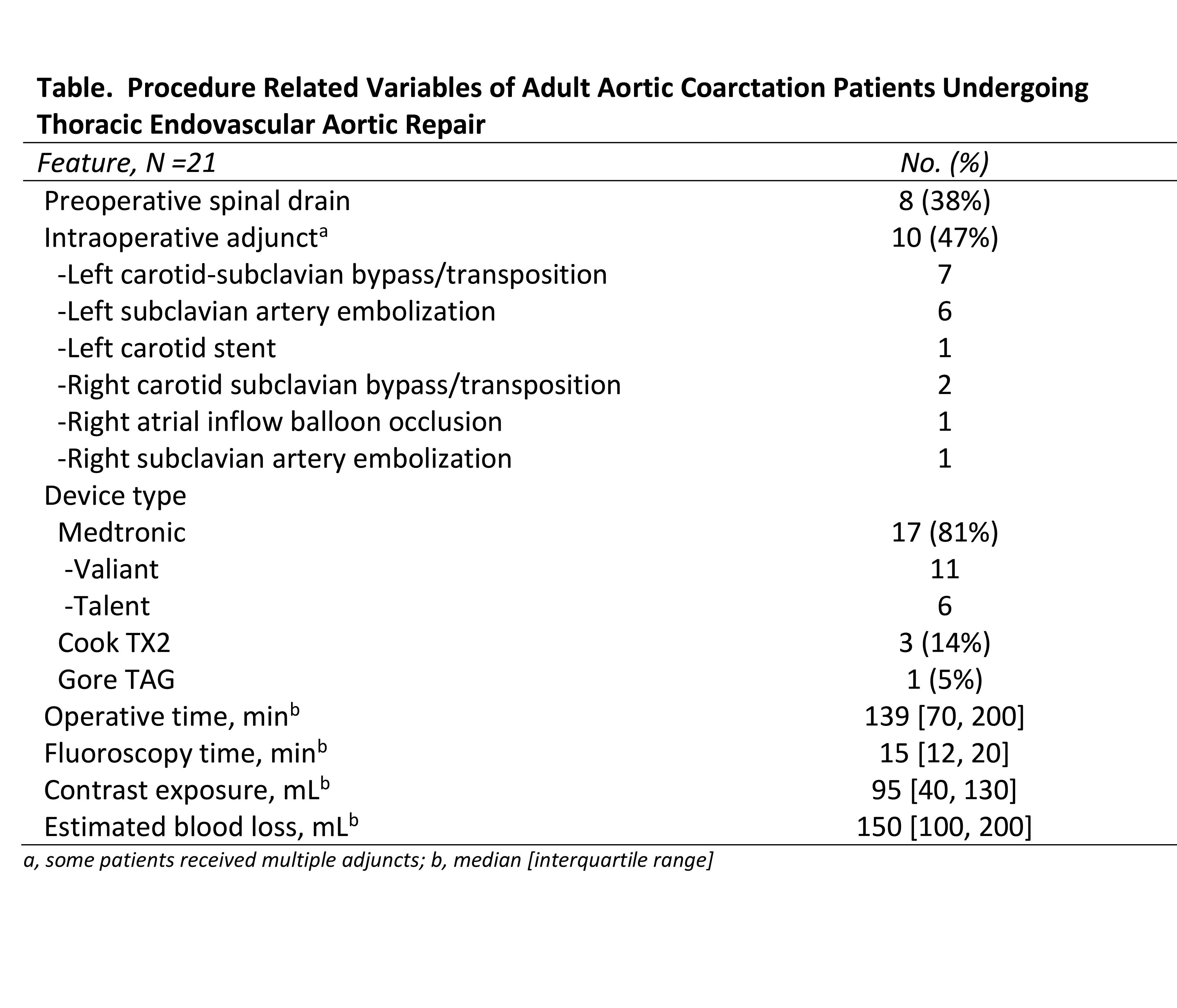
Back to 2017 Annual Meeting Program



