
Back to 2017 Annual Meeting Program
Traumatic Aortic Pseudoaneurysm with Bullet Embolism Following Multiple Gun Shot Wounds
Nicholas M Kunda, Mark L. Keldahl
Advocate Illinois Masonic Medical Center, Chicago, IL
Background:
Traumatic aortic pseudoaneurysm is a rare and life-threatening injury that may not be diagnosed at initial presentation and bullet embolism is a well-known but extremely rare complication of gunshot injuries. A review of the literature revealed multiple case reports describing traumatic aortic pseudoaneurysm and bullet embolism, but no specific guidelines for management.
Clinical Case:
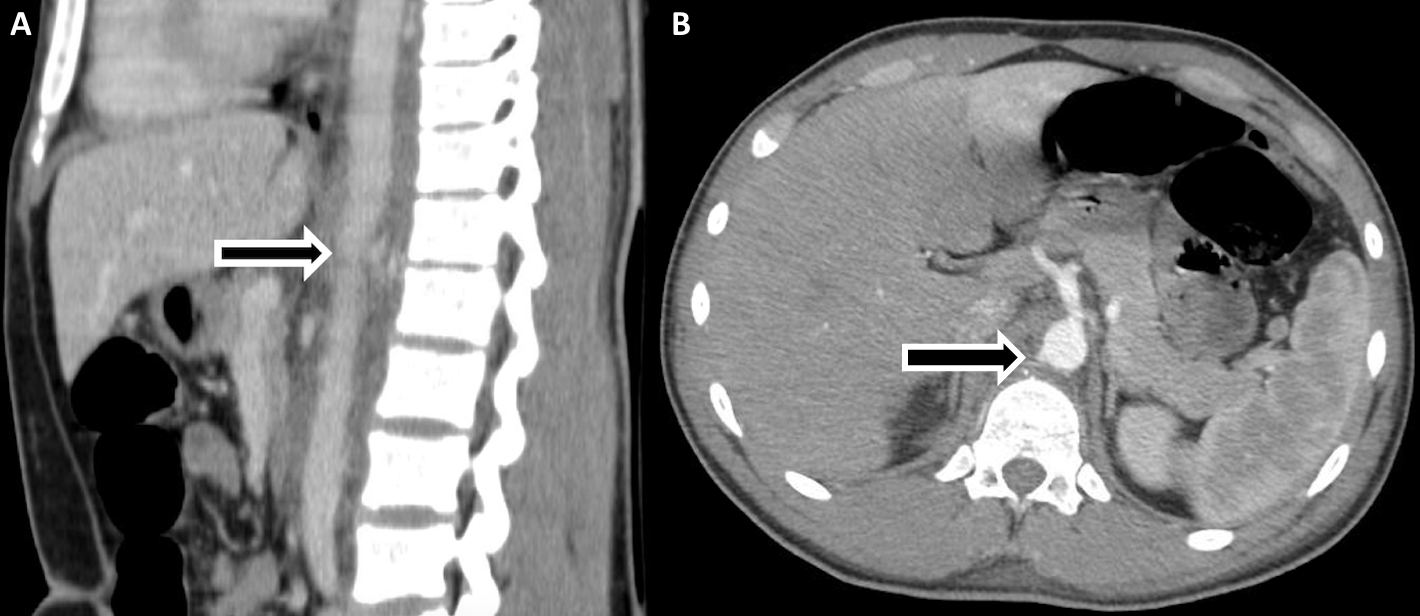
A 19-year-old male was brought to Emergency Department after being shot multiple times in the left arm, left thigh, right forearm, back, and anterior chest. An x-ray of left femur was obtained, showing a retained foreign body posterior to the left patella within the popliteal fossa. On physical exam, the patient was neurovascularly intact with palpable pedal pulses bilaterally. A computed tomography (CT) scan of the chest, abdomen, and pelvis demonstrated a blush posterior to the aorta and anterior to the spine at the level of the 1st lumber vertebrae (L1). A CT Angiogram (CTA) of the abdomen and pelvis showed no active extravasation or pseudoaneurysm formation, however, there appeared to be a small intimal injury adjacent to the L1 fracture. Approximately 3 hours later, the patient began complaining of increased pain in his left knee. A CT of the left lower extremity demonstrated a metallic foreign body within the left popliteal artery. The patient was taken emergently to the operating room for exploration of the popliteal vessels. A Fogarty catheter was used to retrieve the foreign body from the popliteal artery, which was identified as a bullet. After an in depth discussion, it was felt that the bullet must have entered into the aorta at the level of the L1 fracture and embolized distally to the left popliteal artery. A repeat CTA of the abdomen and pelvis was obtained, now approximately 36 hours after initial presentation. This revealed a focal contour abnormality of the right posterolateral wall of the abdominal aorta, just anterior to the 12th thoracic vertebrae (T12), and at the level of the celiac artery. This finding was highly suspicious for post-traumatic pseudoaneurysm formation. The patient was taken back to the operating room for an exploratory laparotomy and open repair of the pseudoaneurysm. Intraoperative aortogram demonstrated the pseudoaneurysm posterior to the celiac artery. The pseudoaneurysm was identified and repaired with a pledgeted Prolene suture.
Conclusion:
Traumatic aortic pseudoaneurysm with bullet embolism is extremely rare and may pose a diagnostic challenge. Although endovascular repair of aortic pathology is becoming more common, open complex aortic surgery is still the standard of care for injuries in such close proximity to the celiac artery. As technology for endovascular stents continues to evolve, vascular surgeons will still need to be familiar with complex exposure and open aortic surgery.

Back to 2017 Annual Meeting Program



