
Back to 2017 Annual Meeting Posters
Outcomes of Resection for Renal Cell Carcinoma with Extensive Inferior Vena Caval Thrombus
Hallie Baer, Georges Haidar, Taylor Hicks, Ronald Rodriguez, Dharam Kaushik, Matthew Sideman, Lori Pounds, Mark Davies
UTHSCSA, San Antonio, TX
Background: Renal cell carcinoma (RCC) has a propensity for vascular invasion with the presence of intravascular tumor thrombus occurring in 10-25% of those cases. Tumor thrombus invades along the renal vein (level 0) to the IVC (level 1-2) and above the hepatic veins (level 3) until ultimately can became an atrial thrombus (level 4), with a worsening prognosis associated with caudal progression. Radical nephrectomy and caval thrombectomy represent the only method of local disease and durable oncologic control. The aim of this study is to examine the outcomes of resection for renal call carcinoma with extensive inferior vena cava thrombus in the setting of a multidisciplinary team.
Methods: A review of a prospectively maintained database of patients with renal cell carcinoma with tumor thrombus was performed. Patients were evaluated pre-operatively with a standardized protocol to assess for extent of disease, specifically presence (and level) of tumor thrombus using renal protocol CT or MRI, as well as evidence of metastases. A multidisciplinary surgical approach was then taken involving Urology, Cardiothoracic, and Vascular surgery. Intraoperative Doppler ultrasound and trans-esophageal echocardiography were performed to aid in confirming the level of thrombus and to identify the lumbar and hepatic veins insertion into the vena cava.
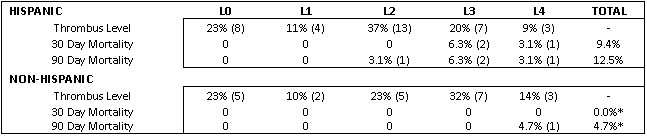
Results: A total of 57 patients underwent radical nephrectomy with tumor thrombectomy over the course of 28 months. Patients were predominantly Hispanic (61%), male (63%), overweight (median BMI 29 [20-56]), and middle aged (median age 58 [21-85]) with a history of hypertension (68%), tobacco use (56%), and diabetes (40%). Almost all patients were symptomatic at presentation: hematuria (53%), flank pain (37%), weight loss (26%). Thrombus level for L0, L1, L2, L3, and L4 disease was 23%, 11%, 32%, 25%, and 11%, respectively. Bypass was required in 35% of cases (veno-veno 25%, cardiopulmonary 11%) and IVC reconstruction with patch only occurred twice (3.5%). Median length of stay was 12 days with a 30-day re-admission rate of 17.5%. Mortality at 30 and 90 days for all patients was 5.7% and 9.4%, respectively.
Conclusions: Renal call carcinoma with extensive inferior vena caval thrombus remains a high risk surgery that requires a multidisciplinary surgical approach, but is associated with acceptable mortality and morbidity. Our results demonstrate Hispanic patients present with less invasive disease than non-Hispanics based on level of thrombus, however Hispanic patients have a higher overall higher mortality at both 30 and 90 days than Non-Hispanic patients.
Back to 2017 Annual Meeting Posters



