
Back to 2017 Annual Meeting Program
Endovascular Treatment of Nutcracker Syndrome: A Case Report
Anthony Rios, Pouria Parsa, John Eidt, Stephen Hohmann, Bradley Grimsley
Baylor University Medical Center, Dallas, TX
Background Nutcracker Syndrome, caused by left renal vein compression as it passes between the superior mesenteric artery and aorta, causes ongoing symptoms ranging from hematuria and orthostatic proteinuria to pelvic congestion syndrome. While an attempt at medical management including aspirin and angiotensin converting enzyme inhibitors works for some, others experience ongoing symptoms. Left renal vein transposition has remained the treatment of choice although endovascular left renal vein stent placement has been advocated in some series with variable success and some complications including stent migration. We present two patients successfully treated with endovascular stent placement with immediate resolution of symptoms, remaining symptom-free after one-year follow-up.
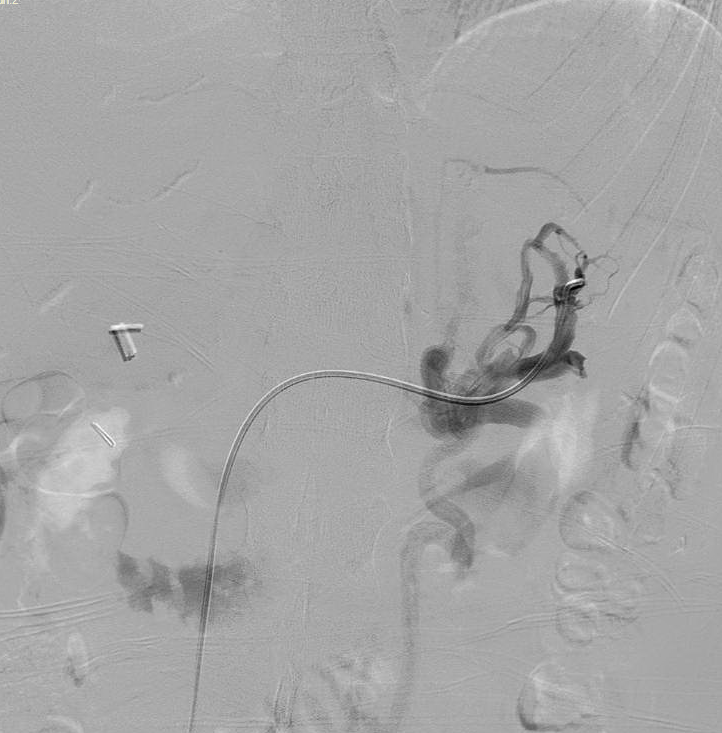
Case Presentation: First is a 32-year-old healthy female presenting with several months of left flank pain causing sleep disruption. She underwent venography, revealing a 90% stenosis of the medial portion of the left renal vein with robust collateral network (Figure 1). The stenotic portion was pre-dilated with a 14 mm x 20 mm high pressure balloon (Armada, Abbott) before placing a 14 mm x 60 mm self- expanding stent (Protege™ GPS™, Covidien) and post-dilating with the same balloon. Completion venography revealed no residual stenosis. Postoperative duplex ultrasound revealed an excellent result with laminar flow and no evidence of stenosis within the left renal vein.
Second is a 48-year-old male with no medical comorbidities presenting with ongoing left flank pain and hematuria. His serum creatinine measured 1.2 mg/dL and a urinalysis revealed 3-5 RBC per high powered field. Venography revealed a 99% stenosis of the medial portion of the left renal vein. The lesion was treated first with angioplasty, using a 14 mm x 20 mm high pressure balloon (Armada, Abbott) before placing a 14 mm x 40 mm self-expanding stent (Protege™ GPS™, Covidien) and post-dilating with a 14 mm x 4 cm angioplasty balloon (XXL™, Boston Scientific). Completion venography revealed no residual stenosis. Flank pain resolved immediately and postoperative computed tomography with intravenous contrast revealed only a small focus of thrombus in the left upper pole renal vein and a widely patent stent.
Conclusions: Our case report confirms Nutcracker Syndrome may be treated through endovascular means, eliminating symptoms and providing a durable alternative to open surgery.

Back to 2017 Annual Meeting Program



