
Socioeconomically Distressed Communities Index Independently PredictsMajor Adverse Limb Events After Infrainguinal Bypass in a National Cohort
Robert B Hawkins, J. Hunter Mehaffey, Eric J Charles, Eric B Schneider, Margaret C Tracci
University of Virginia, Charlottesville, VA
BACKGROUND: Socioeconomic status (SES) is a major determinant of quality of life, as well as life expectancy and healthcare related outcomes. Comprised of factors including financial security, housing, employment and education, SES can be difficult to comprehensively measure limiting its inclusion in large databases. There is a growing interest in the relationship between social determinants of health and outcomes as healthcare shifts from volume to quality-driven metrics. Both community and individual level socioeconomic factors broadly impact surgical morbidity and mortality, although the effect on peripheral vascular disease is not well understood. There is evidence that socioeconomic distress may be a risk factor for peripheral vascular disease as well as increased amputation rates. We sought to determine if the Distressed Communities Index (DCI), a composite socioeconomic score by zip code, could predict outcomes after peripheral vascular surgery. We hypothesized that individuals living in distressed communities as determined by DCI, would demonstrate worse short- and long-term limb related outcomes after infrainguinal bypass.
METHODS: This study included patients from the national Vascular Quality Initiative (VQI) short-term and long-term datasets for patients undergoing infrainguinal bypass (2003-2018). Each dataset was paired with the individual�s DCI score using their home zip code, performed by the database manager such that a de-identified dataset was utilized. The DCI metric was developed by the Economic Innovation Group and is normalized to scale from 0 (no distress) to 100 (severe distress) accounting for unemployment, education level, poverty rate, median income, business growth, and housing vacancies. The DCI is derived from the American Communities Surgery 2014 5-year Estimates and the Census Bureau County and Zip Code Business Patterns. Patients were excluded for missing home zip code and relevant clinical factors.
The primary outcome of interest was the incidence of in-hospital and long-term major adverse limb events (MALE) defined as amputation, revision or thrombectomy. Secondary outcomes included in-hospital major morbidity consisting of acute kidney injury, and pneumonia, as well as major adverse cardiac and in-hospital cerebrovascular events (MACCE) consisting of myocardial infarction, stroke and death. For univariate analysis, patients were stratified by whether they lived in a severely distressed (DCI >75) versus less distressed (DCI ≤75) community. The Chi-Square Test was used to compare categorical variables while the Mann-Whitney U-Test was used to compare continuous variables. Hierarchical generalized linear models assessed the association between DCI and short-term outcomes, while time-to-event analyses assessed long-term results. Risk adjustment accounted for 25 baseline and operative risk factors, year and clustering at the hospital level. For regressions, DCI was scaled for a 25-point change.
RESULTS: A total of 40,109 individuals who underwent infrainguinal bypass had complete short-term data with DCI available, of whom 32,798 also had long-term data available. Patients came from a wide range of communities with substantial between hospital variation in patient DCI scores (Figure). Patients from severely distressed communities are younger, more likely to smoke, disproportionately African American, and have higher rates of medical comorbidities such as hypertension, chronic obstructive pulmonary disease, and diabetes (all p<.05). Patients from distressed communities also had more advanced peripheral vascular disease presenting more commonly with critical limb ischemia (60% vs 56%, p<.0001) and more commonly having prior amputation (6.3% vs 4.7%, p<.0001). There were no differences in elective case status or rate of infrageniculate target, but patients from severely distressed communities received prosthetic conduit more often (43.6% vs 41.8%, p<.0001).
There was no difference in in-hospital mortality (1.3% vs 1.3%, p=.91), 1-year mortality (9.2% vs 9.2%, p=.96), or in-hospital MACCE (3.7% vs 4.1%, p=.06). However, patients from distressed communities had higher rates of in-hospital major morbidity (21.1% vs 18.7%, p<.0001) and MALE (14.4% vs 11.7%, p<.0001). Being from a distressed community was associated with all three component complications, amputation (11.5% vs 9.0%, p<.0001), revision (2.5% vs 2.0%, p<.008), and thrombectomy (3.3% vs 2.8%, p=.013). After risk-adjustment, DCI remained a significant predictor of in-hospital MALE with a 25-point increase associated with a 5% increase in the odds of MALE (95% CI 1.02-1.08, p=.001). Further, DCI remained an independent predictor of amputation after risk adjustment (OR 1.07, 95% CI 1.03-1.10, p<.0001). In models including other socioeconomic status factors, increasing DCI was associated with increased odds of MALE (OR 1.06, 95% CI 1.03-1.09, p=.0005) whereas white race (OR 0.86, 95% CI 0.80-0.92, p<.0001) and private insurance (OR 0.62, 95% CI 0.57-0.67, p<.0001) were both associated with reduced risk of in-hospital MALE.
Long-term MALE remained elevated in patients from severely distressed communities (1-year Kaplan-Meier estimate 30.1% vs 26.8%, p<.0001), with a 44.8% greater incidence of amputation (16.1% vs 11.2%, p<.0001) and a 14.5% greater incidence of thrombectomy (7.7% vs 6.7%, p=.005). After risk-adjustment, DCI continued to independently predict long-term MALE (HR 1.02, 95% CI 1.00-1.04, p=.045). DCI was also associated with risk-adjusted amputation (HR 1.09, 95% CI 1.05-1.12, p<.0001) and occlusion with a hazard ratio of 1.04 (Table). Patients from severely distressed communities were significantly more likely to identified as active smokers on long-term follow-up 31.6% vs 25.3%, p<.0001).
CONCLUSIONS: Patients from severely distressed communities (DCI>75) demonstrated higher rates of smoking and comorbid disease. Additionally, these patients presented with more advanced vascular disease, including critical limb ischemia and prior amputations. While in-hospital mortality and cardiovascular events were similar between groups, the rate of major morbidity was higher in patients from highly distressed communities. Moreover, patients from distressed communities demonstrated increased risk of major adverse limb events both in hospital and long-term. Moreover, the novel Distressed Communities Index was found to be an independent predictor of MALE after adjusting for baseline and operative risk. Amputation was the main driver of this finding and DCI independently predicted in-hospital and long-term amputation. All available socioeconomic measures including DCI, insurance status and race were associated with short-term limb events.
Socioeconomic factors play an important role in vascular surgical outcomes, in particular limb related events. This is likely due to an interdependent combination of individual means and community level resources. The DCI related associations observed in this study warrant further investigation. Identifying modifiable risk factors may help mitigate the increased risk of adverse events through preoperative risk-factor optimization and close follow-up. Based on the link with outcomes and high variability between hospitals, any future attempts at risk prediction and public reporting of quality should consider socioeconomic factors. The Distressed Communities Index can be easily integrated into databases in a de-identified manner to help account for socioeconomic status. 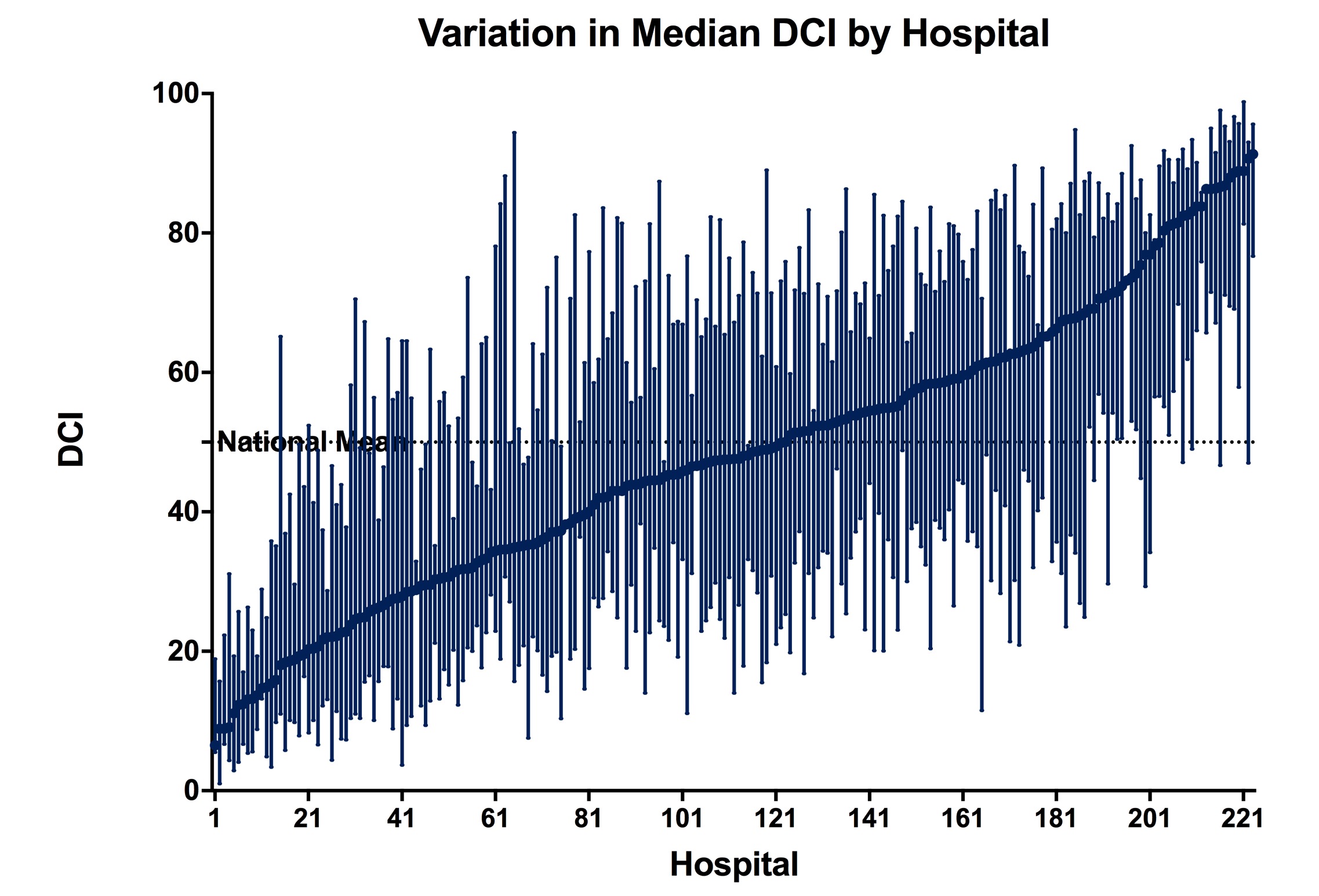
| HR | 95% CI | p-value | AHR | 95% CI | p-value | |
| MALE | 1.04 | (1.02-1.06) | .0005 | 1.02 | (1.00-1.04) | .045 |
| Amputation | 1.14 | (1.11-1.18) | <.0001 | 1.09 | (1.06-1.12) | <.0001 |
| Revision | 0.99 | (0.96-1.02) | .472 | 0.99 | (0.96-1.02) | .383 |
| Thrombectomy | 1.05 | (1.01-1.10) | .009 | 1.03 | (0.98-1.07) | .221 |
| Occlusion | 1.09 | (1.05-1.12) | <.0001 | 1.04 | (1.00-1.07) | .028 |
Back to 2019 Abstracts