
Determining the True Preference of Applicants Dual Applying to Surgical Specialties: Is the 0+5 Integrated Vascular Residency the Backup?
Katherine McMackin1, Nicholas Hoell2, Joseph Lombardi1
1Cooper University Hospital, Camden, NJ; 2Cooper Medical School of Rowan University, Camden, MD
Background: Many applicants dual apply to different surgical specialties. Level of interest in a specialty is consistently cited as one of the most important factors for program directors when evaluating applicants for 0+5 integrated vascular surgery programs (IVS). The purpose of this study was to examine trends in dual application submission and to determine the percentage of applicants to integrated vascular residencies with vascular as their true preference.
Methods: Electronic Residency Application Service (ERAS) Statistics for non-international medical graduates from 2011 to 2017 were mined for trends in dual applications between integrated vascular surgery and the other surgical specialties. The dual application percentage, range, and standard deviation were determined. National Residency Match Program (NRMP) Results and Data from 2011 to 2018 was also used to identify those US Seniors who ranked vascular integrated programs as their preferred choice - defined as ranking vascular as the only choice or the first-choice specialty, compared to those who raked a specialty other than vascular first. This data was also collected for applicants to orthopedic surgery, neurosurgery, otolaryngology, obstetrics and gynecology, integrated cardiothoracic surgery and integrated plastic surgery.
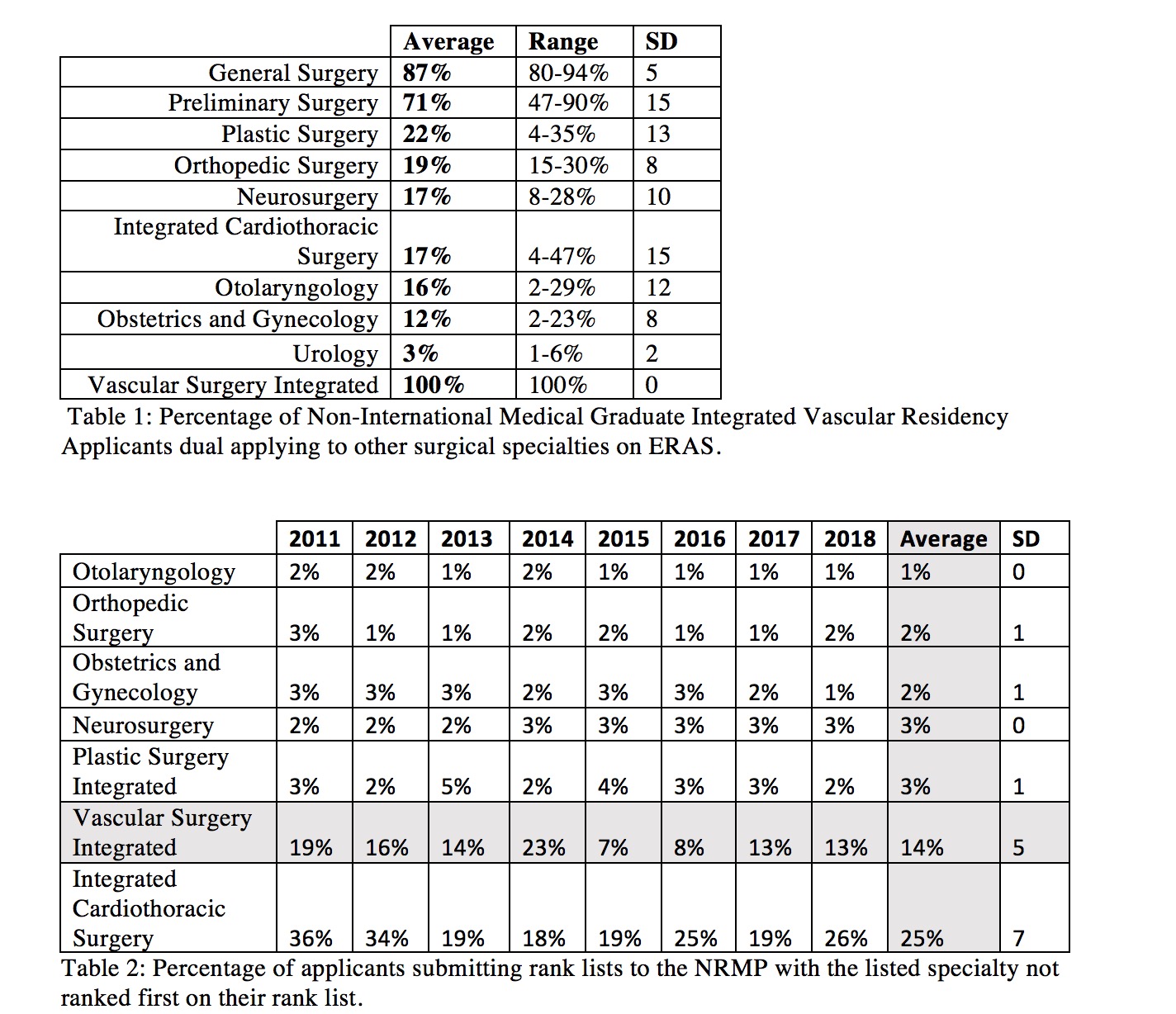
Results: Between 2011 and 2017, applicants who applied to IVS most often dual applied to IVS and general surgery (87%) followed by IVS and :preliminary surgery (71%), plastic surgery (22%), orthopedic surgery (19%), neurosurgery (17%), otolaryngology (16%), obstetrics and gynecology (12%), and urology (3%) (Table 1). Dual applications to IVS and integrated cardiothoracic surgery showed the greatest variability over this time period, range 4-47% SD 15. Dual applications to IVS and urology showed the least variability, range 1-6% SD 2. Between 2011 and 2018, an average of 14% of IVS applicants who submitted rank lists to the NRMP ranked a specialty other than vascular as their first preference (range 7-23 SD 5). Only integrated cardiothoracic surgery had a higher percentage of applicants listing a different specialty as their true preference at 25% (range 18-36 SD 7). Nearly all (97-99%) applicants to orthopedic surgery, neurosurgery, otolaryngology, obstetrics and gynecology, and plastic surgery applied to that specialty as their true preference (Table 2).
Conclusions: Integrated vascular residency applicants were most likely to dual apply to general and vascular surgery. Compared to the other surgical specialties, those who submitted rank lists to the NRMP for cardiothoracic and IVS had the highest likelihood of ranking another specialty higher. Care must be taken when evaluating applications to integrated vascular residencies to determine the applicant’s level of interest in vascular surgery as a career.
Back to 2019 Posters