
Trends in Use of Cerebrospinal Drains and Outcomes Related to Spinal Cord Ischemia in the Vascular Quality Initiative
Victoria Aucoin1, Bolanle Bolaji1, Zdenek Novak1, Emily Spangler1, Danielle Sutzko1, Graeme McFarland1, Benjamin Pearce1, Scali Salvatore2, Adam Beck1
1University of Alabama at Birmingham, Birmingham, AL;2University of Florida, Gainesville, FL
BACKGROUND: Spinal cord ischemia (SCI) is a feared complication of aortic repair. Given that cerebrospinal fluid (CSF) drain placement has some inherent risk, but also known benefit, a better understanding of CSF drain practices and utilization in prevention and treatment of SCI is needed to guide use. We utilized the Vascular Quality Initiative (VQI) database to identify trends in CSF drain usage and SCI rates in thoracic endovascular aneurysm repair (TEVAR) and complex branched/fenestrated endovascular aneurysm repair (cEVAR). We also sought to evaluate differences in outcome in patients who developed SCI despite preop drains vs those treated with therapeutic postop drains (ie selectively drained).
METHODS: We evaluated elective TEVAR/cEVAR for aneurysm from 2014-2020 in the VQI; trauma, dissection, aneurysm from dissection, PAU & IMH were excluded. CSF drain use over time, factors associated with prophylactic vs therapeutic drain placement in those with any SCI (transient and/or permanent), and outcomes related to these groups were evaluated by χ2 analysis, and survival differences assessed by Kaplan-Meier analysis.
RESULTS: 3,469 TEVAR/cEVAR procedures met all criteria with an overall SCI rate of 2.5% (88/3469), which decreased from 4.55% in 2014 to 1.43% in 2018. Prophylactic drain use remained relatively stable (30% in 2014 to 27% in 2018); aortic coverage extent also remained consistent over time.
Among the subset that developed SCI, demographics and prior history (including CAD, HTN, CHF, DM, CKD, and COPD) were not significantly different between preop prophylactic drain patients compared to postop therapeutic drain patients. Prior aortic surgery was significantly more common among patient with preop prophylactic drains compared to postop therapeutic (46.2% vs. 23%; p= .019). Procedure time was longer in patients requiring therapeutic drains for SCI compared to those with prophylactic drains developing SCI (mean 290 min vs. 183 min; p < .01). Postop therapeutic drains were also associated with postop MI (8% vs 0%; p= .047). A higher in-hospital mortality was seen in patients with therapeutic drains compared to prophylactic preop CSF drain placement, but did not reach statistical significance (16% vs 33%; p= .11). Total and postop lengths of stay were non-significantly longer with preop drain use. Survival analysis among SCI patients revealed decreased survival in patients who had postop therapeutic drains placed (Figure).
CONCLUSIONS: SCI rates have decreased over time, although prophylactic CSF drain use has remained unchanged in the VQI. Among SCI patients, long-term survival was dramatically lower in patients suffering SCI requiring postop therapeutic drains compared to those who developed SCI with a preop prophylactic drain in place. Similar to MI or CVA where time to intervention for rescue matters, patients with therapeutic drains may fare worse than prophylactic drain patients due to increased delays in decreasing CSF pressure leading to secondary spinal cord injury. This and the survival advantage seen with prophylactic drains even in patients suffering SCI, should give surgeons pause when considering a selective drain policy. 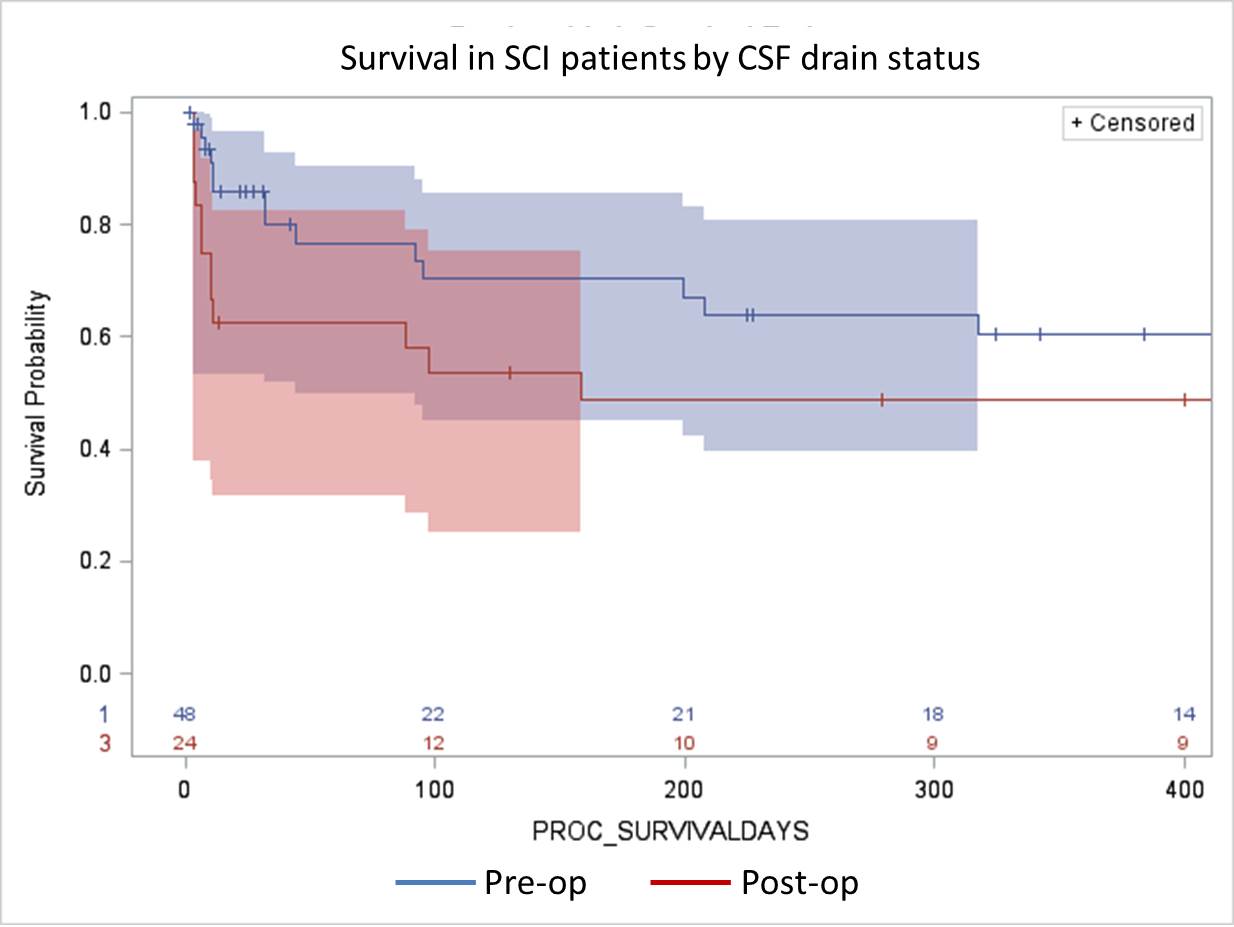
Back to 2020 Abstracts