
Distal Revascularization and Interval Ligation for Dialysis Access-Related Ischemia is Best Performed Utilizing Arm Vein Conduit
M. Libby Weaver, Courtenay Holscher, Alexis Graham, Thomas Reifsnyder
Johns Hopkins Hospital, Baltimore, MD
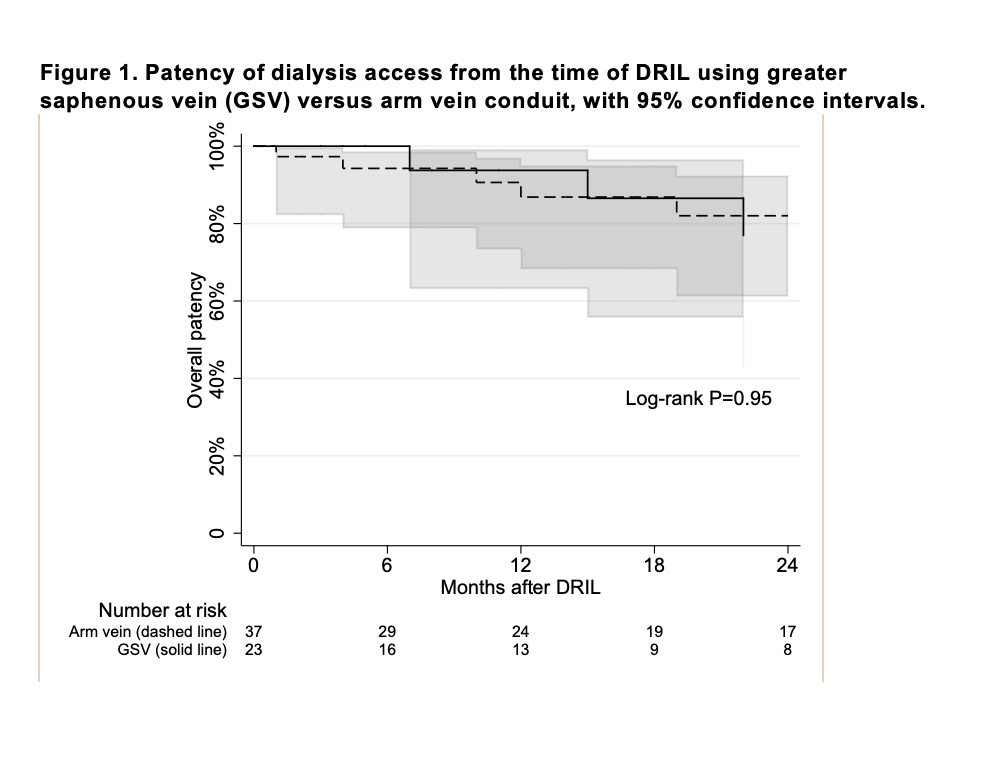
BACKGROUND: Distal revascularization and interval ligation (DRIL) is an effective approach to management of hemodialysis access-related ischemia that offers both symptom relief and access salvage. Greater saphenous vein (GSV) is the most commonly utilized conduit. However, the GSV harvest site can be particularly high risk for post-operative wound complications, especially in patients with risk factors such as obesity and diabetes. Additionally, if ipsilateral arm vein is available and used as the conduit then a general anesthetic can be avoided. The aim of this study is to determine the suitability of DRIL utilizing arm vein as compared to GSV conduit by comparing outcomes including symptom relief, access salvage, and wound complications. METHODS: All patients who underwent DRIL between 2008 and 2020 were retrospectively identified in the electronic medical record. Characteristics and outcomes of those with arm vein versus GSV conduit were compared using Wilcoxon log-rank and chi-square tests. Access patency was examined using Kaplan-Meier methods, with censoring at loss to follow-up or death. Additionally, we examined post-operative outcomes of wound complications, resolution of steal symptoms, need for ligation of access, and DRIL bypass patency. A wound complication was defined as any presentation requiring an intervention, such as antibiotic treatment or debridement. RESULTS: 66 patients who underwent a DRIL procedure for hand ischemia were included in the study. Arm vein conduit was utilized in 40 patients (median age 65 years, 25% male) and GSV conduit in 26 patients (median age 58 years, 19% male). Basilic vein was the most commonly used arm vein (83%). There were no significant differences in comorbid conditions between the two groups, with the exception of diabetes mellitus (DM) (78% arm vein vs 50% GSV, P=0.02). Most patients were obese (50% and 60% in the GSV and arm vein conduit groups respectively). Nearly half of all patients had a history of tobacco use and coronary artery disease, and nearly 1/3 had a history of peripheral arterial disease. The dialysis access in most patients was an arteriovenous fistula, with less than 20% of patients presenting with steal syndrome secondary to a graft. On average, patients presented with steal 4 months after access creation. There was no difference in ischemia stage at presentation between the groups, with most patients presenting with stage 3 ischemia (Table 1). There was no difference in primary or primary-assisted patency of hemodialysis access following DRIL by arm vein vs. GSV conduit (P=0.92, P=0.95 respectively). At 12 and 24 months after DRIL 86.9% (95% CI 68.3%-94.9%) and 82.0% (95% CI 61.3%-92.3%) of patients with arm vein conduit maintained access patency compared to 93.8% (95% CI 63.2%-99.1%) and 76.9% (95% CI 43.0%-92.2%) of those with GSV conduit (Figure 1). All but one patient had partial or complete resolution of symptoms. Wound complications were significantly greater in the GSV as compared to the arm vein conduit group (46% vs 11%, P=0.001). DRIL bypass remained patent in all but one patient in each group at a mean follow-up time of 25 months (0-112 months). Access ligation was required in 2 patients with DRIL using GSV conduit, and in one with DRIL using arm vein conduit. Only one of these ligations, in the GSV group, was for ongoing ischemia. The other two were for infection, and post-transplant without further need for dialysis, respectively. Three patients required minor amputation, the most serious of which was a ray amputation of the fifth digit of the hand. CONCLUSIONS: DRIL is an effective management strategy for dialysis access-related steal syndrome that relieves ischemia while avoiding access abandonment. DRIL procedures utilizing arm vein have advantages over those performed with saphenous vein. In our series, symptom resolution, fistula patency, and bypass patency were equivalent, but there were distinctly fewer wound complications, with only 11% of patients in the arm vein conduit group developing post-operative wound complications despite a high rate of risk factors for surgical site infection, including obesity, diabetes, and tobacco use, in this cohort. Additionally, utilization of arm vein conduit avoids the need for the use of general anesthetic. This series of patients undergoing DRIL using arm vein conduit is the largest series to date, and no prior studies have directly compared outcomes of DRIL using arm vein versus GSV conduit. There may be reluctance among surgeons to use arm vein conduit in order to preserve autogenous options for future dialysis access if needed. However, our data demonstrates excellent patency of existing access post-DRIL. If ipsilateral arm vein is available it should be considered the conduit of choice when performing distal revascularization and interval ligation. 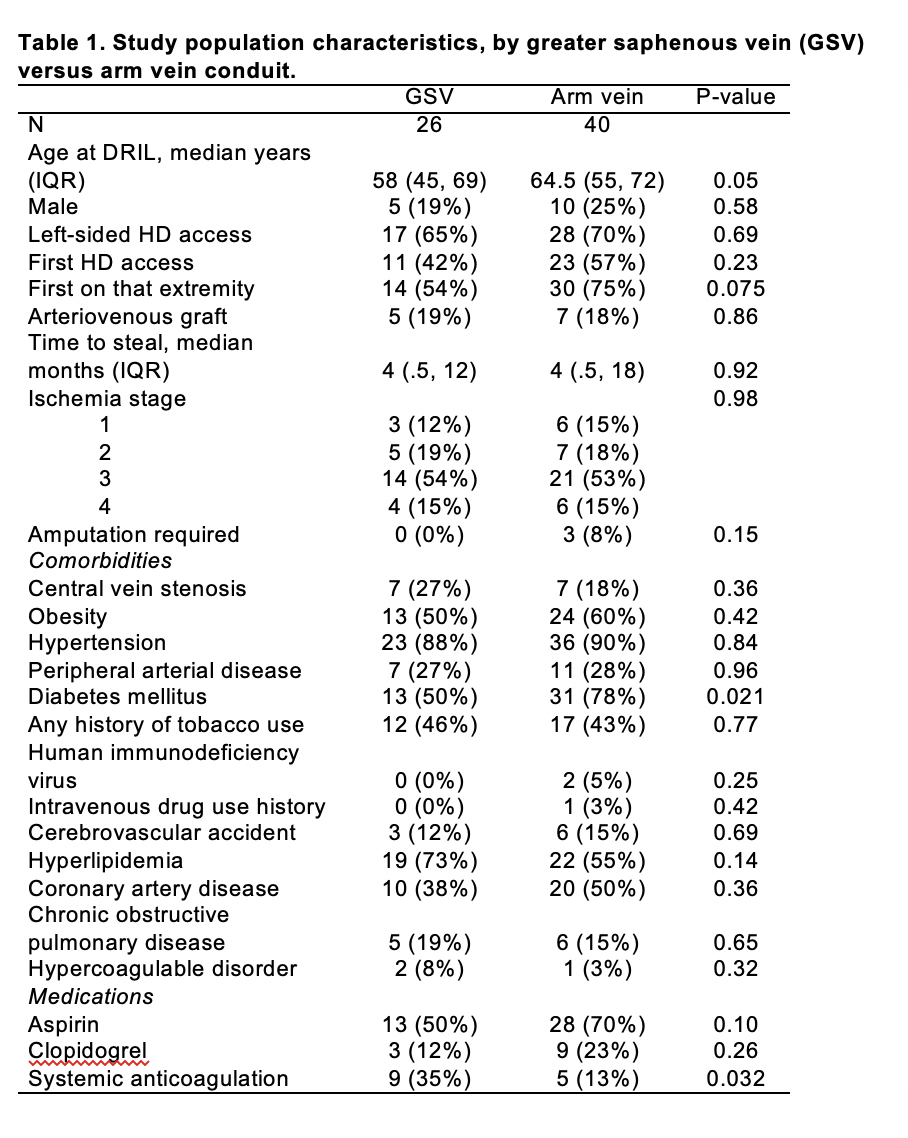
Back to 2020 Abstracts