
Implications of Aortic Remodeling on Re-intervention and Survival after Endovascular Repair of Chronic Type B Aortic Dissection with Aneurysm
Dean J. Arnaoutakis, Tabassum A. Khan, Salvatore T. Scali, Kristina A. Giles, Michol Cooper, Scott A. Berceli, Thomas S. Huber, Gilbert R. Upchurch, Jr., Martin Back
University of Florida, Gainesville, FL
Background: Controversy exists surrounding thoracic endovascular aortic repair(TEVAR) of chronic type B dissection(cTBAD) due to concerns about durability. Entry tear coverage to induce false lumen(FL) thrombosis is thought to be an important determinant of subsequent aneurysm regression; however, septum compliance and distal re-entry tear retrograde FL perfusion coalesce to promote a dynamic remodeling environment between the true and FL. There is a paucity of literature describing the influence of early remodeling events on subsequent risk of re-intervention and survival for cTBAD. The purpose of this analysis was to investigate early aortic remodeling events after TEVAR for cTBAD and determine how they are associated with re-intervention and survival.
Methods: All cTBAD patients undergoing TEVAR from 2005-2017 at a single institution were reviewed. Three-dimensional centerline analysis was performed on sequential preoperative and postoperative imaging up to 2 years postoperatively. Segmental phenotyping of the dissected thoracoabdominal aorta included characterization of postoperative FL thrombosis, as well as true lumen(TL)/FL and total aortic diameter changes. Early(6-month postoperatively) positive aortic remodeling(PAR) was defined by a 5% reduction in maximal thoracic aortic diameter. Kaplan-Meier analysis was used to estimate freedom from re-intervention and overall survival.
Results: A total of 95 patients(mean age 61±12 years; 90%-male; BMI 30±6) were identified(median follow-up 20[IQR 4, 49]months). Dissection extension into the visceral segment was present in 90%(n=85) and mean preoperative maximal thoracic diameter was 63±11mm. The proportion of total and thoracic aortic coverage was 47±12% and 73±16%, respectively. In-hospital mortality was 1.1%(n=1; no 30-day death) after the index TEVAR(any SCI 4%;permanent-1%)(retrograde dissection-1%).
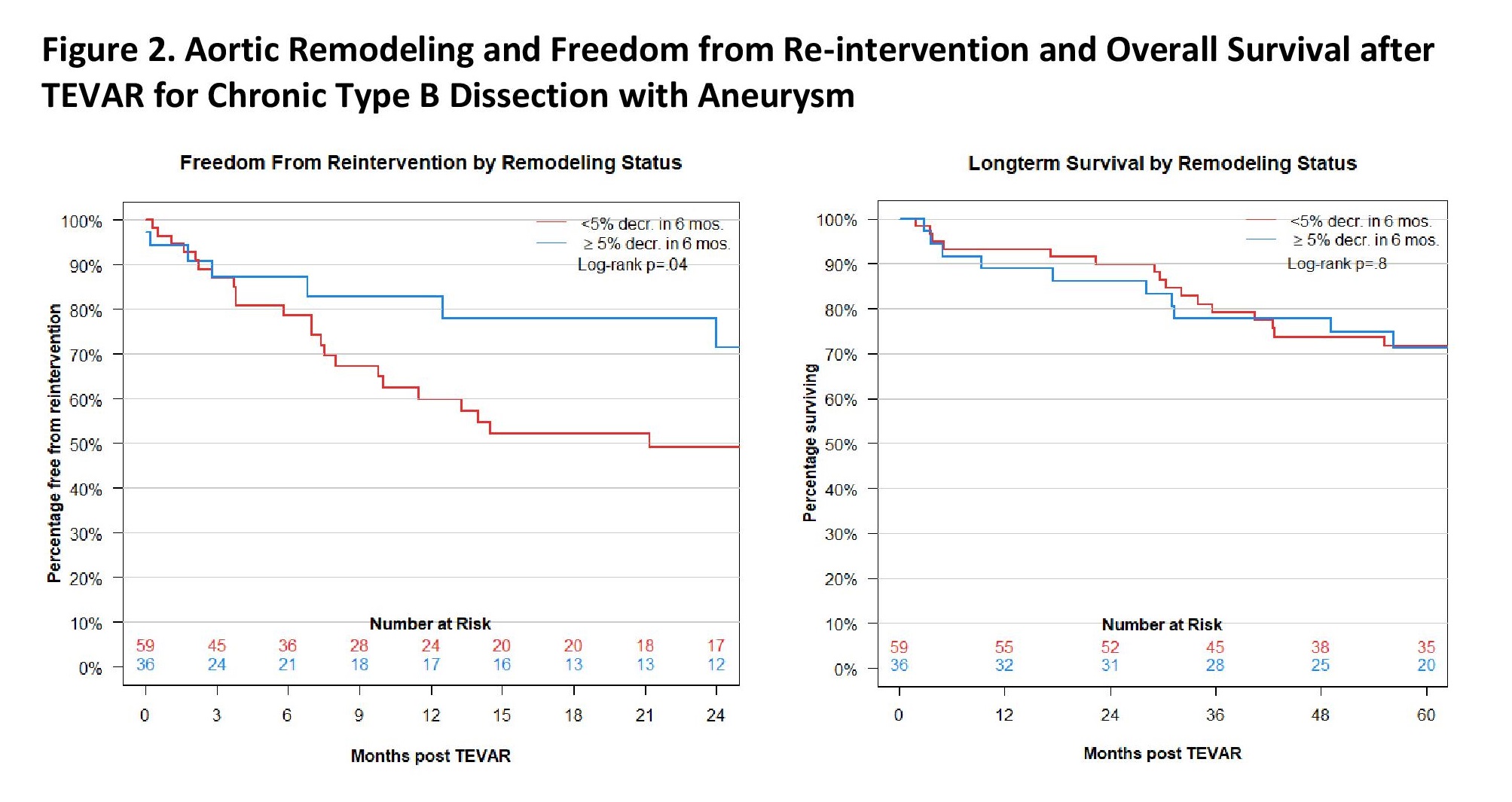
Thoracic FL thrombosis occurred in 71%(n=67) while abdominal FL thrombosis occurred in 60%(n-57) by 6-months. A 5% decrease in maximal thoracic diameter occurred in 38%(n=36) during this interval. From preprocedure through 2 years, there was an overall increase in TL diameter and concomitant decrease in FL diameter at the level of the largest diameter in both the thoracic and abdominal aorta for patients experiencing PAR(Figure 1). The overall rate of aortic re-intervention was 39%(n=37; non-elective-37%). A majority of re-interventions occurred within the intended treatment zone(n=22 of 37) due to persistent FL perfusion and/or proximal/distal stent extension to manage attachment site endoleak and/or fenestrations while the remaining involved the distal thoracoabdominal aorta. The 1 and 3 year freedom from re-intervention was significantly lower in subjects experiencing early PAR(log-rank p=.04). Patients experiencing re-intervention did not have different survival compared to those without re-intervention. Similarly, overall survival was not different between patients with or without PAR(log-rank p=.8)(Figure 2).
Conclusions: Early PAR events are associated with decreased rates of re-intervention; however overall survival is not impacted by these changes. TEVAR for cTBAD results in a high rate of re-intervention which should be discussed preoperatively with patients and mandates vigilant surveillance protocols postoperatively. 
Back to 2020 Abstracts