
Mycotic Right Subclavian Artery Aneurysm: A Rare and Challenging Pathology
Lily Fatula1, Tyler Fleming2, Brian Jones1, Christopher Carsten1
1Prisma Health System Upstate, Greenville, SC;2University of South Carolina School of Medicine Greenville, Greenville, SC
INTRODUCTION: Subclavian artery aneurysms (SAAs) are uncommon, constituting less than 1% of peripheral artery aneurysms. Mycotic subclavian aneurysms only account for 6.5% of these making them exceedingly rare. Presentation may be subtle until the aneurysms are quite large and present with compressive, ischemic, or hemorrhage symptoms. The location of these aneurysms and their etiology make treatment challenging and outcomes uncertain. We present the case of a 67-year-old hemodialysis patient who presented with cough, dysphagia, and recurrent bacteremia secondary to a mycotic right SAA.
METHODS: This patient’s history was significant for R sternoclavicular and sacroiliac septic arthritis. The patient had experienced multiple episodes of Methicillin sensitive staph aureus (MSSA) bacteremia. Echocardiogram was negative for endocarditis. She was treated with several courses of antibiotics including vancomycin, nafcillin, and cefazolin. After months of repeated therapy, the patient presented with the above complaints. Chest X-ray demonstrated a large paratracheal mass. CT angiogram of the chest confirmed the presence of a large aneurysm of the proximal right subclavian artery. The decision was made for operative repair. Preoperative assessment included blood cultures, infectious disease consult, echocardiogram, nuclear medicine stress test, and coronary angiography. Due to the location of the aneurysm it was not felt amenable to endovascular repair. The location also raised concern for difficult proximal control and the potential need for cardiopulmonary bypass, thus cardiothoracic surgery was involved.
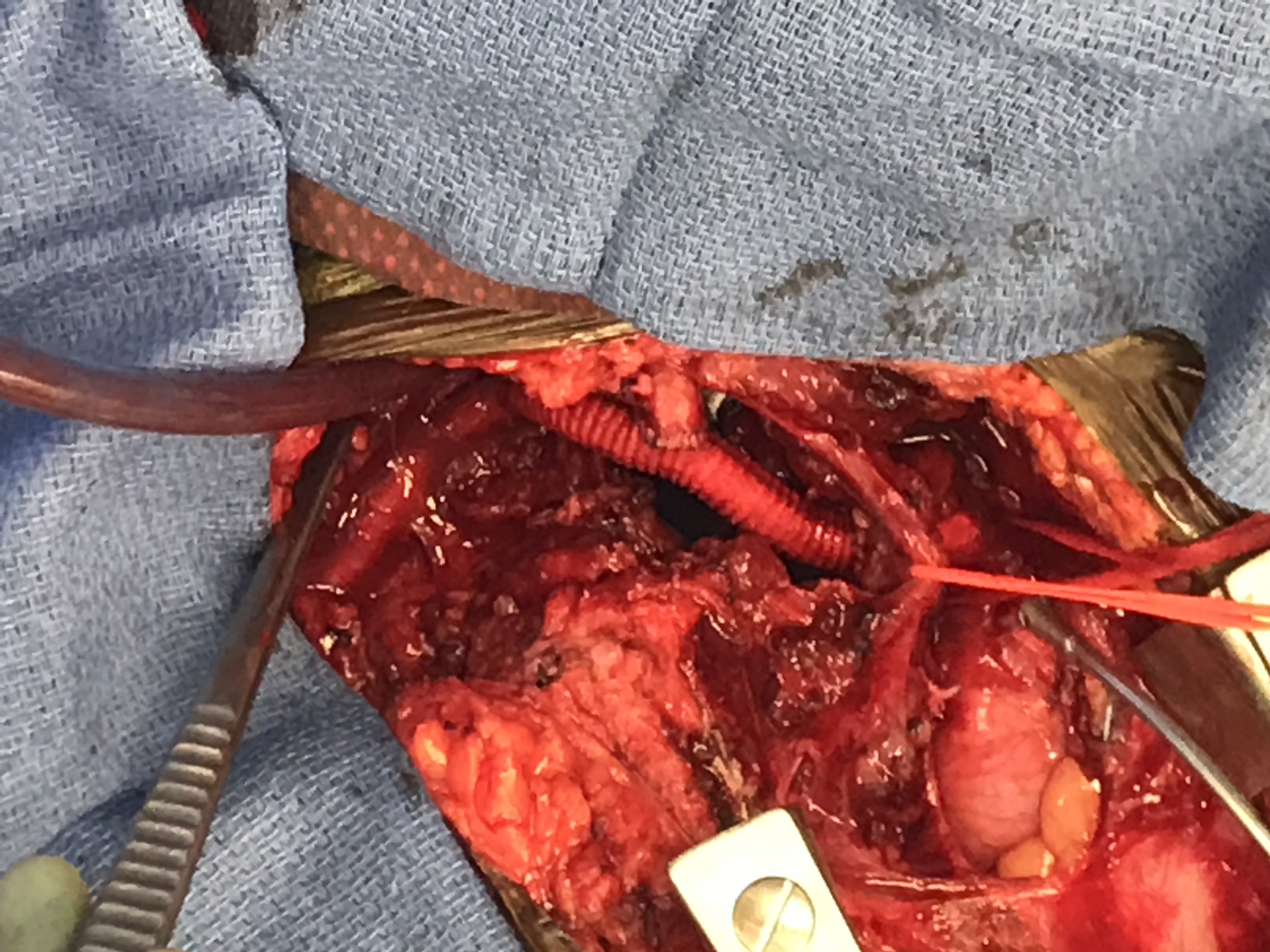
RESULTS: The patient underwent open surgical repair of the right SAA using rifampin-soaked Dacron. A median sternotomy and infraclavicular incision with clavicular resection was performed. Because the patient had chronic venous occlusion involving both the subclavian veins and the superior vena cava, a large bore sheath was placed in her arteriovenous thigh graft for intra-operative resuscitation. An anatomic revascularization was performed with common carotid re-implantation. The patient made an uneventful recovery and has remained free of recurrent bacteremia on life-long suppressive antibiotics.
CONCLUSIONS: Mycotic subclavian artery aneurysms represent a rare and challenging pathology that may require a collaborative approach to treatment. 
Back to 2020 Abstracts