
“Impact bilateral carotid body tumor resection in the carotid baroreceptor function”
Santiago Mier y Teran-Ellis1, Humberto A. Estrada-Rodriguez1, Javier E. Anaya-Ayala1, Gabriel Lopez-Pena2, Emmanuel A. Contreras-Jimenez1, Xelha A. Domiguez-Vega1, Alejandra A. Gonzalez-Duarte1, Carlos A Hinojosa3
1Instituto Nacional de Ciencias Medicas y Nutricion "Salvador Zubiran", Mexico, Mexico2Instituto Nacional de Ciencias Medicas y Nutricion "Salvador Zubiran", Tlalpan, Mexico3Instituto Nacional de Ciencias Medicas y Nutricion "Salvador Zubiran", Mexico city, Mexico
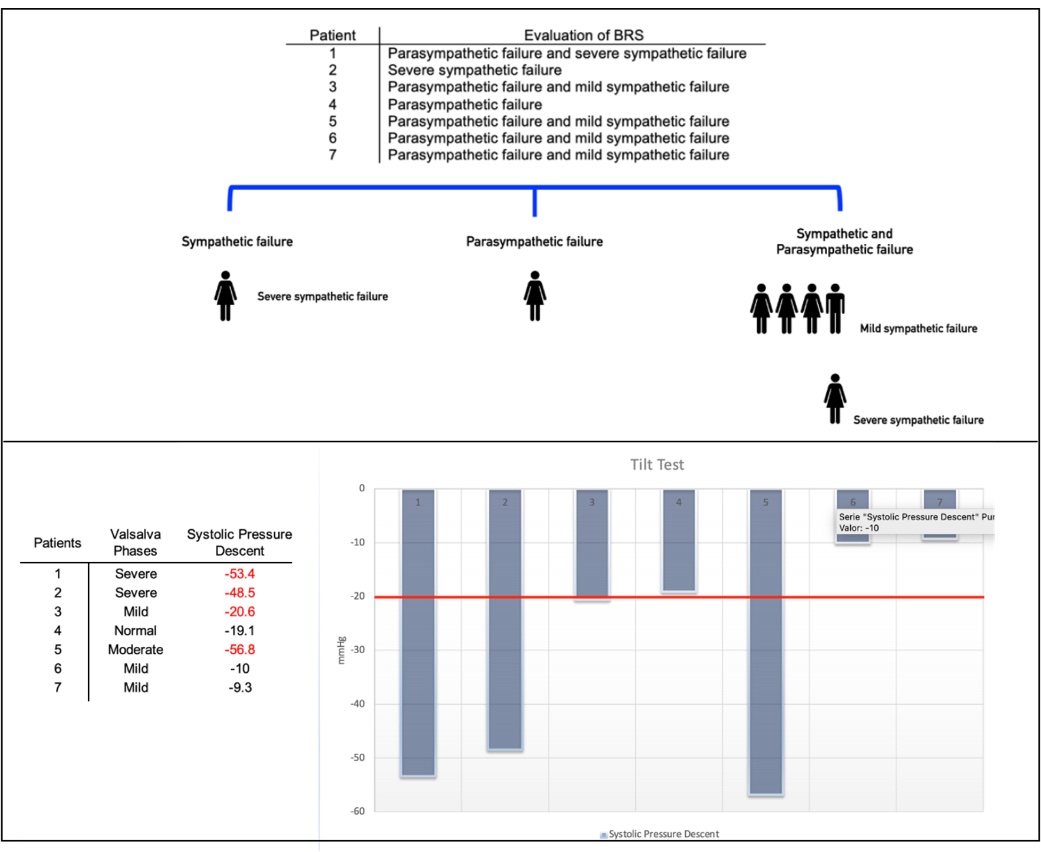
Background: Baroreflexes are responsible for maintaining blood pressure (BP) homeostasis and avoiding volatile hemodynamic changes. The baroreflex arc is a negative feedback loop that acts as a buffer for BP and heart rate during postural changes, physical or emotional stress. When some afferent component of this arc fails, prompting changes in the function of the baroreceptors, it is known as baroreceptor failure (BRF). Four forms of presentation have been described: hypertensive crisis, volatile hypertension, orthostatic malignant vagotonia. It may occur after extensive cervical surgery, radiation and trauma. To our knowledge no previous study has quantified BRF after the surgical treatment of bilateral Carotid Body Tumor.Methods: A prospective cohort of patients that underwent carotid body tumor (CBT) resection at our institution underwent preoperative and postoperative evaluation. Baroreceptor sensitivity (BRS) was assessed in patients with bilateral CBT resection recording symptomatology associated to BRF, or history of BP variability. Baseline demographic characteristics, clinical and a quantitative evaluation of baroreceptor sensitivity was conducted using the Composite Autonomic Severity Score (CASS).Results: From our institutional database that include a total of 144 patients (151 resections), 7 patients with bilateral tumors were identified (Table 1). Mean age 61 years (SD±11), six females (85%); none of them had family history of paragangliomas. Only one of 14 resected CBTs had malignant histopathological characteristics (7%). Patients main complaint was asymptomatic cervical mass in five cases (71%), the remainder with odynophagia (29%). In regards, immediate postoperative events: only one patient had an episode of bradycardia, leading to a 40 seconds asystole, no etiology was identified. After the contralateral CBT excision, three BRF events occurred (43%); two patients presented with volatile hypertensive crisis and one with supraventricular tachycardia. Regarding baroreceptor sensitivity (Figure 1), it was found in all seven patients (100%). Most common symptoms were syncope, vertigo and fatigue (57%); palpitations (28%) and one orthostatic headache. BRF characteristics found are as follows: five patients (71%) had mixed condition. In four of them, qualitatively, it was classified as mild, and in one patient as severe. Of the other 2 patients; one had severe sympathetic failure and one had parasympathetic dysfunction. All patients were diagnosed with BRF (100%), four were previously diagnosed with generalized anxiety disorder and, in none of the seven patients was ever a suspicion baroreceptor dysfunction as etiology.Conclusions: Baroreceptor failure after bilateral CBT surgery is an underestimated and underdiagnosed clinical sequela and possible complication, its incidence remains unknown. BRF can range from volatile hypertensive crisis, severe bradycardia or asystole in immediate postoperative period, to syncope, vertigo and fatigue which appears several weeks later, the most frequent condition is the mixed, sympathetic and parasympathetic. Further studies are necessary to predict this postoperative change when planning CBT resection.
Figure 1: Evaluation of baroreceptor sensitivity.
| Patient | Gender/Age (Years) | Comorbities | Headache | Palpitations | Syncope | Fatigue | Vertigo |
| 1 | F/51 | None | Yes | Yes | Yes | Yes | |
| 2 | F/65 | Pituitary adenoma | Yes | Yes (Mild) | |||
| 3 | F/83 | Antiphospholipid Syndrome | Yes | Yes | Yes | ||
| 4 | F/68 | Essential Tremor | Yes (Severe) | ||||
| 5 | F/60 | Obstructive Sleep Apnea, Obesity | Yes | Yes (Severe) | Yes | ||
| 6 | M/44 | Obstructive Sleep Apnea | Yes (Severe) | Yes | |||
| 7 | F/58 | None | Yes | Yes |
Back to 2022 Abstracts