


Open Repair of an Abdominal Aortic and Right Common Iliac Artery Aneurysm without Genetic Disorder in a 19-Month Infant
Khalil Chamseddin, Antonio Solano, Melissa R Keller, Michael C Siah, Gerardo Gonzalez-Guardiola, Michael Shih, Vivek Prakash, Carlos H Timaran, Shadman Baig, Melissa L Kirkwood
University of Texas Southwestern Medical Center, Dallas, TX
INTRODUCTION: Abdominal aortic aneurysms (AAA) in pediatric patients are a rare clinical condition. Commonly described etiologies include infection, vasculitis, connective tissue diseases and trauma. However, idiopathic AAA are even more atypical. We report a unique presentation of a pediatric patient with incidental findings of AAA and right common iliac artery (CIA) aneurysm found during workup for heart failure (HF) treated with open aneurysm repair.
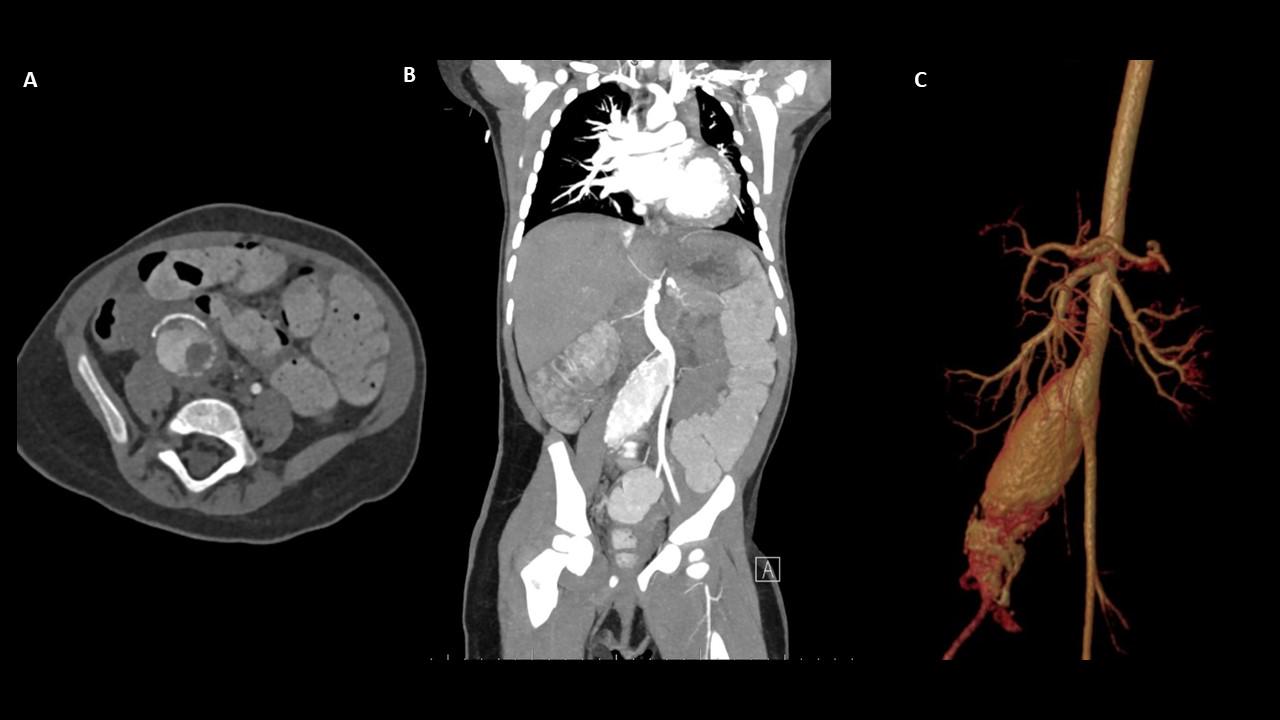
METHODS: A 19-month-old female presented with dyspnea, emesis and abdominal pain to the emergency department. Initial workup chest X-ray revealed right lobe pulmonary effusion and cardiomegaly. Extension studies demonstrated dilated cardiomyopathy with concomitant HF and pulmonary embolism. Given the persistence of severe hypertension, an abdominal computerized tomography angiogram was performed, with evidence of right kidney atrophy, a 4-cm infrarenal AAA with intraluminal thrombus and a 2.6-cm right CIA aneurysm. The patient was transferred to our institution where extensive genetic testing was performed and only positive for secondary carnitine deficiency. The patient’s HF and extreme drug resistant hypertension was medically optimized for three weeks in the cardiac care unit prior to open surgical repair.
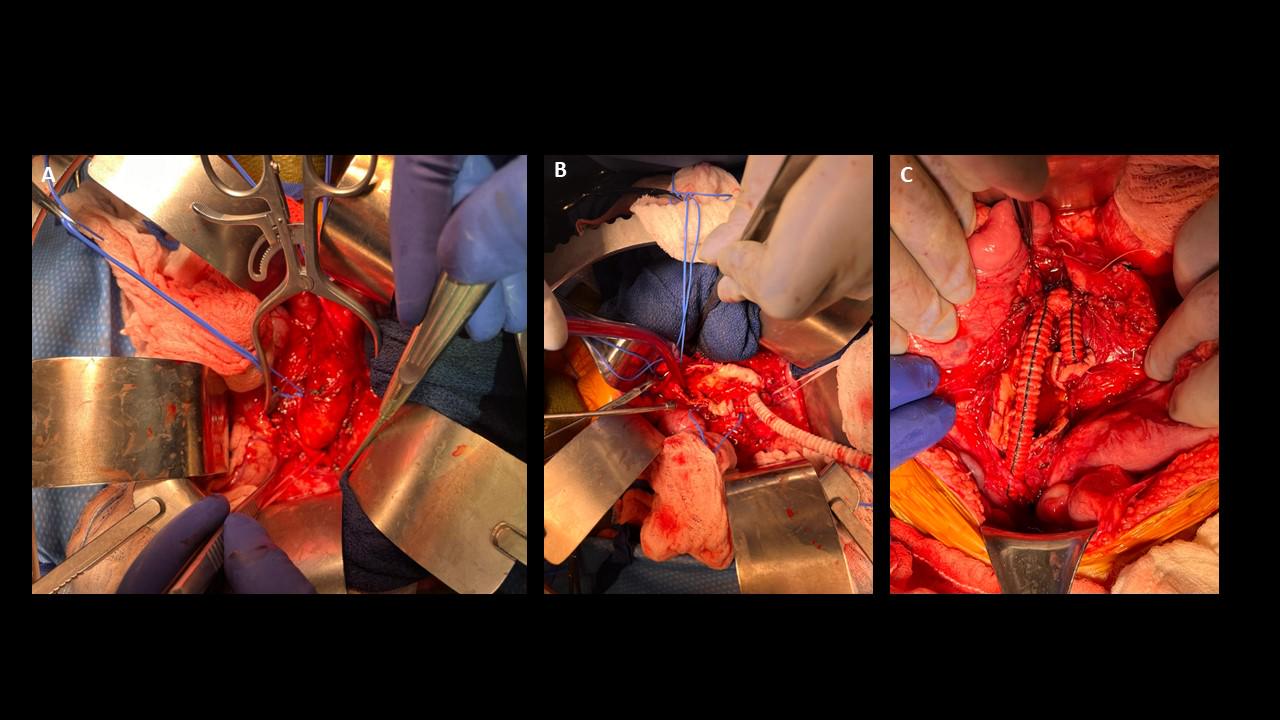
RESULTS: An aortic bi-iliac artery bypass with a 12 x 6 mm Dacron graft (Maquet Cardiovascular, LLC, Wayne NJ) from the infrarenal aorta to the right external iliac artery and left CIA was performed. The inferior mesenteric artery was preserved and the right internal iliac artery was ligated. The patient tolerated the procedure well, with immediate postoperative improvement of blood pressure and cardiac function. Surgical pathology from the excised aortic tissue findings were negative for active vasculitis and demonstrated fibrotic thickening of the aortic tunica intima and media, and luminal thrombus with dystrophic calcification. At 30-day follow-up, she achieved complete recovery and was only on one oral hypertensive medication.
CONCLUSIONS: Aortic and iliac artery aneurysms are a rare treatment challenge in infants. We report the sixth case of a concomitant infrarenal AAA and iliac aneurysm in a pediatric patient without known genetic causes. We considered idiopathic retroperitoneal fibrosis as a potential etiology given the dense inflammation noted in the retroperitoneum, however no hydronephrosis was present. Our patient remains a diagnostic challenge who will need lifelong follow up for further aneurysmal degeneration.
Back to 2024 Abstracts