


Extensive Pelvic Aneurysms in a Patient with Giant Cell Arteritis
Drew Braet, Matthew J Corriere
University of Michigan, Ann Arbor, MI
INTRODUCTION: A 38 year-old male with history of cryptogenic strokes and diffuse aneurysmal disease presented with worsening left leg pain, numbness, and weakness with computed tomography angiogram (CTA) demonstrating extensive left pelvic aneurysms.
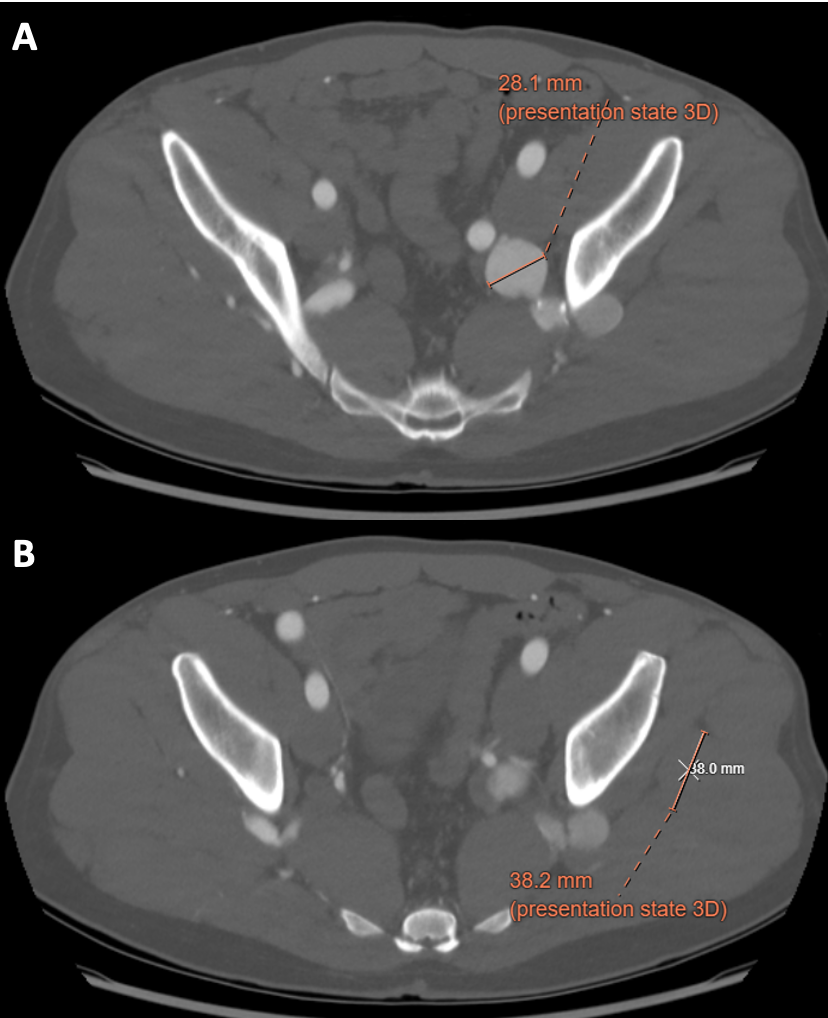
HISTORY: The patient had previously been managed at an outside center for visceral artery, bilateral common iliac, and common femoral artery (CFA) aneurysms. He previously underwent open repair of his splenic and superior mesenteric artery aneurysms. Extensive workup for auto-immune, vasculitis, and connective tissue disorders was negative. After establishing care at our center for surveillance, he reported worsening left leg pain, numbness, and weakness. CTA demonstrated extensive left superior and inferior gluteal artery aneurysms (GAA) (maximum diameter of 2.9 cm, Fig 1A) and a 3.8 cm distal saccular aneurysm located outside the pelvis (Fig 1B). We offered him an GAA embolization with stent graft exclusion of left internal iliac artery (IIA). PLAN: Via percutaneous left CFA access we selectively catheterized and coil embolized the left inferior GAA, superior GAA, and IIA aneurysm. A embolization plug and covered stent graft was were used to exclude the IAA. Completion angiogram demonstrated successful exclusion of the IAA. However, a focal segmental occlusion of the tibial vessels was noted. We elected to perform an embolectomy with repair his left CFA aneurysm. Fresh thrombus was retired and segment of CFA aneurysm was sent to pathology. His post-operative course was uneventful, with improvement in his buttock and leg pain. He was discharged on post-operative day two on Xarelto and aspirin. His intra-operative pathology revealed smoldering giant cell arteritis (GCA).
DISCUSSION: GCA is a granulomatous vasculitis of unknown origin that affects large and medium sized arteries. Temporal arteritis (cranial GCA) is characterized by headache, jaw claudication, and visual symptoms. Extracranial GCA is rare and manifests exclusively in large arteries, most commonly involving the aorta, subclavian, and/or cerebral arteries. Although inflammatory changes have been identified in the femoral and iliac vessels, to our knowledge there is no report of femoral and/or GAA in patients with GCA. Herein we present a novel case of a patients with GCA who has extensive aneurysmal disease and pelvic aneurysms.
Back to 2024 Abstracts